Mayo clinic 3d printing
3D Anatomic Modeling Laboratories - Overview
People undergoing new, uncommon or complex surgeries at Mayo Clinic may benefit from access to the clinic's expertise in 3D anatomic models. This technology helps with surgical planning, patient education and medical education.
The 3D anatomic modeling laboratories of the Department of Radiology use 3D printing to help doctors tailor the treatment of adults and children based on their exact anatomy. Studies in peer-reviewed medical journals show that the use of 3D-printed models improves surgical outcomes.
Anatomic modeling laboratories are available at the clinic's campuses in Arizona, Florida and Minnesota. Mayo Clinic is a leader in the movement to bring this technology into hospitals for the benefit of all people.
3D printing of patient's anatomy aids in surgical planning
At Mayo Clinic, radiologists and surgeons are teaming up to discover every possible detail about complex cases, before the operation. Use of virtual modeling and 3D-printed models can mean that patients experience less pain, shorter hospital stays and quicker recoveries.
How it works
3D Printing for Cancer Treatment
Click here for an infographic to learn moreAccurate 3D anatomic models are based on people’s imaging results, such as CT or MRI scans. Before printing a 3D model, radiologists process the scans with sophisticated software to first create a virtual model color coded for each tissue type. Then one or more printer technologies are used to print, layer by layer, a life-size 3D model of the patients' anatomy.
The printer's jetting technology uses UV light to harden thin layers of liquid resin as it builds the structure one layer at a time. Most models are printed in plastic. Sometimes they're made of flexible materials so that surgeons can practice a surgical technique on a more lifelike model.
Applying technology to personalize treatment
3D printing can be a valuable tool for surgeons, who may use a 3D anatomic model specific to a patient to explain, plan or even practice surgery. During the digital preparation stage before printing, doctors may use the images for virtual surgical planning. After printing, being able to hold the anatomic model before beginning surgery may help in understanding anatomic anomalies or additional information that may change the surgical approach.
During the digital preparation stage before printing, doctors may use the images for virtual surgical planning. After printing, being able to hold the anatomic model before beginning surgery may help in understanding anatomic anomalies or additional information that may change the surgical approach.
Isaac Garcia's story: Bone cancer care at Mayo Clinic
A team-based approach
Innovating with 3D anatomic models
Surgeons use the point-of-care manufacturing capabilities of the Mayo Clinic 3D anatomic modeling laboratories to conduct surgical rehearsals next to the operating room.
At Mayo Clinic nearly every medical and surgical specialty has accessed and benefited from the services of the anatomic modeling laboratories and the 3D models they produce. These specialties include pediatric otorhinolaryngology (ear, nose and throat), orthopedic surgery, oncologic surgery and cardiovascular surgery. Surgeries for which 3D-printed anatomic models are proved to be helpful include head and neck surgery, complex facial or airway reconstruction, heart surgery, lung surgery, joint reconstruction, and tumor removal.
These 3D models also play an important role in education and are used by Mayo Clinic's medical students, residents, fellows and experienced surgeons learning new or uncommon procedures.
Innovating with 3D modeling
The anatomic modeling laboratories:
- Have produced more than 6,000 models
- Produced Mayo Clinic's first model in 2006 to help the surgical team plan a complex surgery to separate conjoined twins
- Created models that have become the standard of care for multiple uses, including jawbones that have guided over 100 jawbone removals (mandiblectomies) and 300 hearts
Mayo Clinic physicians, scientists and engineers continually advance the study and practice of 3D modeling in surgery.
Research and innovation
Mayo Clinic experts in 3D anatomic modeling conduct research to develop new solutions that improve treatment. See a list of publications about 3D anatomic modeling by Mayo Clinic researchers on PubMed, a service of the National Library of Medicine.
See physician staff
Point-of-care additive manufacturing provides complex scoliosis models
March 27, 2021
Mayo Clinic has the largest point-of-care additive manufacturing facility in the United States. The 8,000-square-foot space provides highly accurate 3D-printed anatomic models and surgical guides for Mayo's surgical specialists.
"Our manufacturing facility is located in our hospital within the Department of Radiology, so we can easily interact with surgeons. We're able to move rapidly from customized CT and MRI protocols to the creation of a patient-specific, life-sized 3D-printed models or devices," says Jonathan M. Morris, M.D., a neuroradiologist and medical director of the 3D Anatomic Modeling Laboratory at Mayo Clinic in Rochester, Minnesota.
The models are valuable presurgical and intraoperative tools for the treatment of adults with complex scoliosis. "Holding a 3D model makes it much easier to understand complex anatomy, particularly in revision surgeries or in patients with congenital adult scoliosis," says Jeremy L. Fogelson, M.D., a neurosurgeon specializing in spinal care at Mayo Clinic in Rochester, Minnesota. "When we look at 2D images on a screen, we see one slice at a time and then have to do a lot of mental juggling to reconstruct those slices into a real-life image."
Fogelson, M.D., a neurosurgeon specializing in spinal care at Mayo Clinic in Rochester, Minnesota. "When we look at 2D images on a screen, we see one slice at a time and then have to do a lot of mental juggling to reconstruct those slices into a real-life image."
Dr. Fogelson cites a case in which a 3D spinal model indicated that an adult scoliosis surgery would be more complex than he initially thought. "The patient was a man with very large bones. An X-ray can't show you bone size," Dr. Fogelson says. "But when I held the model, I realized we needed to operate over two days in order to safely work through that much tissue."
Mayo's model-manufacturing process starts with CT and sometimes volumetric MRI, using imaging protocols designed by Mayo Clinic radiologists specifically for 3D printing. A Mayo radiologist evaluates the accuracy of the imaging data before the model is produced.
"Our patient-specific models aren't developed only according to an algorithm created by an engineer who doesn't fully understand anatomy," Dr. Morris says. "The biomedical engineers in our facility are part of the clinical care team, routinely working with radiologists and surgeons."
Morris says. "The biomedical engineers in our facility are part of the clinical care team, routinely working with radiologists and surgeons."
Customized patient models
Customized patient models
Jeremy L. Fogelson, M.D., a neurosurgeon specializing in spinal care at Mayo Clinic in Rochester, Minnesota, examines a 3D-printed spinal model in the operating room.
The imaging data is segmented, and the model is created using several 3D printers. "No single printer does it all — we have the capability to do additive manufacturing using all seven ASTM standards," Dr. Morris says. "The life-sized model we give to the surgeon is exactly what the surgeon is going to find during the patient's procedure."
Mayo Clinic launched its additive manufacturing facility in 2005. Mayo's campuses in Arizona and Florida also have 3D anatomic modeling laboratories as of 2020, with collaboration occurring enterprisewide.
As a tertiary center, Mayo Clinic performs a high volume of revision surgeries for adults with complex scoliosis. The 3D imaging protocols use advanced techniques such as iterative metal artifact reduction and multispectral energy to reduce artifacts from metal implants. "Without those techniques, we don't get an accurate model," Dr. Morris says.
The 3D imaging protocols use advanced techniques such as iterative metal artifact reduction and multispectral energy to reduce artifacts from metal implants. "Without those techniques, we don't get an accurate model," Dr. Morris says.
The 3D models can enhance the safety of revision procedures, which are often performed in the absence of anatomic landmarks removed during the patient's original procedure. "It can be challenging to determine optimal screw placement in a revision spine with bone grafts," Dr. Fogelson says. "Examining the 3D model before surgery — rotating it and looking at the side of the spine that will remain covered during the surgery — guides our screw locations and trajectories. We also save time in the operating room because at times we don't need additional imaging or technology to guide screw placement."
Mayo Clinic performs 3D printing in numerous materials, including sterilizable materials for use in the operating room. Planning is underway for printing on titanium through Mayo Clinic Engineering.
"That will allow us to innovate and serve more patients with unique needs," Dr. Morris says. "Our goal is to provide complex, customizable models and guides that benefit our patients, who come to Mayo for solutions they can't get anywhere else."
For more information
3D Anatomic Modeling Laboratories. Mayo Clinic.
Exclusive interview with Dr. Jonathan Morris, Mayo Clinic Radiologist
Reading time: 6 min.
Jonathan Morris3D printers will soon be able to print everything from custom implants to life-size mock-ups of organs. The possibilities of 3D printing of CT or MRI images open up exciting prospects for radiology and healthcare in general.
For Dr. Jonathan Morris , neuroradiologist at the Mayo Clinic who specializes in spinal work, the bright future of medical 3D printing is today. He and his fellow radiologist Dr. Jane Matsumoto co-leads the 3D Printing Lab and is at the forefront of bringing this innovative technology into practice.
We asked Dr. Morris about how often 3D printing is used at the Mayo Clinic in Rochester, Minnesota, USA, in which cases it is most applicable, what hinders the wider use of 3D printers in clinics, and why he argues that this direction should develop under the auspices of radiology.
– How useful is 3D printing for the Mayo Clinic?
– In medicine, it is not uncommon for us to have to surgically remove an organ or part of it and replace it with something. 3D printing is often invaluable in such cases.
The 3D printing process begins with a scan of the patient's body on a CT or MRI machine. We load the resulting data into the medical CAD software and then color-code the piece we want to print using a process called segmentation. After that, we save the resulting image in an SDL file and export it to the printer. To make it clear: one CT scan of the entire spine can consist of 5,000 images, so converting such a volume of information for 3D printing requires significant computing power.
In Mayo, we started by making individual preoperative models for patients with mandibular tumors. On such a model, we plan in advance all the necessary incisions and actually print guides for them, which are screwed to the patient's bone before the operation. This reduces the time spent in the operating room, improves the outcome of treatment and reduces the cost, which, ultimately, is extremely important for medicine.
In addition, one of our world-class vascular surgeons has come up with a new way to apply 3D printing to his field. He works with bypass stent companies, but sometimes none of the designs available on the market fit. Therefore, we began to print aortas for specific patients with aneurysms, developing into individual solutions for each.
Vascular surgeons with our help have become easier to deal with complex cases of stenting. How does this happen? We take the CT scan results and convert them into a 3D model that fully matches the patient's anatomy, and then perform a future interventional procedure on it. You could say we are "simulating" the patient. This makes it possible to train doctors: residents, interns and medical trainees, to perform any manipulations without the direct participation of the patient.
You could say we are "simulating" the patient. This makes it possible to train doctors: residents, interns and medical trainees, to perform any manipulations without the direct participation of the patient.
– How did you start using 3D printing in your clinic?
- Eleven years ago, Siamese twins were admitted to the Mayo Clinic. The surgeons asked us if we could make a 3D model of their liver because the anatomy of the patients was quite unusual and the doctors had to choose how to divide the organ. Traditionally, such a decision is made using CT and MR scans. The results of these studies are a two-dimensional visualization, and sometimes it is not easy to build a three-dimensional object in the imagination.
At least because the image size of the scanned object corresponds to the screen size. If you are displaying it on your iPhone, the object will be the size of the palm of your hand. If on a 40ft screen during a large conference, it will immediately "grow" to 40ft. It is difficult to imagine realistic scales based on 2D renderings.
It is difficult to imagine realistic scales based on 2D renderings.
We undertook to make a 3D model, but at that time we didn't have our own 3D printer. So we used a local college printer. Dr. Matsumoto has been actively involved in the creation of twin diagnostic imaging because she understands anatomy like no one else.
In the photo: The patient is holding a 3D model of the chest with a tumor.
This year we made about 500 or 600 models for preoperative planning. From the spine, we switched to oncology with tumor resection. If a neurosurgeon is dealing with a large neoplasm in the spine that involves the surrounding blood vessels, we create a holistic model of the entire area. This allows surgeons to plan the operation and compare different methods of its implementation.
After the Siamese twin incident, we started using 3D printers from the engineering department. The Mayo hospital system has 60 engineers and they have several setups that we used in the beginning to make models for spinal surgery. This turned out to be so useful for the surgeons that we decided to get a printing facility based on the hospital, which was an innovation at the time. Only the Walter Reed National Military Medical Center did something similar.
This turned out to be so useful for the surgeons that we decided to get a printing facility based on the hospital, which was an innovation at the time. Only the Walter Reed National Military Medical Center did something similar.
– Which surgeon uses 3D printing the most?
- There are many surgeons in Mayo who specialize in different fields, and many of them are the actual movers of our development. They come and say: “I want to take out the tumor in such and such a location, but through a small incision. Can you make me a model?
From the very first model to today, 3D printing helps advance surgical planning. It allows you to get together, say, an orthopedic surgeon, as well as his colleagues specializing in the problems of the gastrointestinal tract, gynecology, and discuss a specific medical case, having before your eyes the problematic part of the patient's body in full size.
I operate on children with scoliosis, so at first we created spine models for more complex patients. In the end, all surgeons of the clinic appreciated this approach. They began to realize that this was not only convenient for the doctor in preoperative planning, but also useful for patients. Using 3D visualization, it is possible to clearly explain to patients what is wrong with them or their child.
In the end, all surgeons of the clinic appreciated this approach. They began to realize that this was not only convenient for the doctor in preoperative planning, but also useful for patients. Using 3D visualization, it is possible to clearly explain to patients what is wrong with them or their child.
– What problems did you face while creating the program?
- Printers require ventilation. They work with polymers, so there must be an air extractor in the room. The infrastructure of hospitals is not designed for such systems, so we are now working with specialists to re-equip the premises.
Our 3D model production now covers thousands of square feet. We're doing this not just for Rochester, but for healthcare facilities throughout Mayo. We launched print programs at additional locations in Jacksonville, Florida and Scottsdale, Arizona. But the main production is located here. Instead of installing 3D printers everywhere, we decided to take a centralized approach.
Since we entered the 3D medical printing market at an early stage, we had to develop quality control programs to ensure the accuracy of the image. You must be sure that the printer prints objects of the correct size. Working with the Society of Manufacturing in Engineering and groups using 3D printing in other industries, we have created all the necessary standards. Error in surgery is of the utmost importance, and if we send something the wrong size to the operating room, it could be fatal. Therefore, from the very beginning of the work of the laboratory, we have been especially focused on quality and safety.
Pictured: Anatomically accurate Mayo Clinic 3D model
While we don't get compensation for 3D models, Mayo's principle is that the best interests of the patient come first. At first, we printed all models for free, but as evidence was collected that their use improves treatment outcomes, we decided to offer this service to the market.
– How will 3D printing develop?
– Talented surgeons are needed to use this technology. 3D printing is another tool at their disposal to be innovative. With the help of models, they can perform operations that would otherwise be impossible, make surgical interventions less invasive and achieve better results.
3D printing is another tool at their disposal to be innovative. With the help of models, they can perform operations that would otherwise be impossible, make surgical interventions less invasive and achieve better results.
We have been working with the FDA (Food and Drug Administration) for the last three years to help develop regulations. Once 3D models are used to make medical decisions, the process needs to be regulated.
Ultimately we will try to develop standards for cost recovery. The Japanese healthcare system is funding the use of 3D models in cancer treatment, and England is also starting to consider paying. So this will happen someday with us, there is no doubt.
In addition, there are still many bottlenecks in 3D printing. Segmentation software is inconvenient from a clinician's point of view as it is intended primarily for engineers. For example, you can get an image of an adult bone in just a few clicks. But if we want it to be with arteries, veins, a tumor, segmentation will take four hours. I think the development of software will follow the path of increasing the efficiency of 3D printing in complex cases in oncology and cardiology.
I think the development of software will follow the path of increasing the efficiency of 3D printing in complex cases in oncology and cardiology.
The next step is to print the scaffold that you place in the body for the bone to grow along it. Such tests have already been carried out on large animals and will soon be carried out on humans. There are attempts to print leather. Being able to bioprint bones, cartilage, or at least the scaffold along which they will grow, is a big deal.
We firmly believe that 3D printing should be developed under the umbrella of radiology. Radiologists have the best understanding of diagnostic imaging, the best knowledge of anatomy, and the best understanding of where tumors are located. We should be the ones doing segmentation. If 3D printers are popping up like mushrooms in every department without quality checks, it will lead to an out of control process. And in the end - to medical errors.
3D printed anatomical models for preoperative planning and enhanced patient consent
Introduction
3D printed models are becoming increasingly useful tools in the modern practice of personalized, precision medicine. As case histories become more complex and treatments become truly unique, visual and tactile anatomical models can improve understanding and communication in the process of creating a solution for a particular patient.
As case histories become more complex and treatments become truly unique, visual and tactile anatomical models can improve understanding and communication in the process of creating a solution for a particular patient.
Health care professionals, institutions and organizations around the world use 3D printed anatomical models as reference tools for preoperative planning, intraoperative imaging and calibration or pre-positioning of medical equipment for routine and high complexity procedures, which has been documented in hundreds of publications1. Physicians often save time preparing and performing surgeries, resulting in significant reductions in operating costs while reducing patient risk, anxiety, and recovery time.
This guide provides practical step-by-step guidance for physicians and technologists to move from patient scans to 3D printed models by learning how to set up a CT/MRI scan, segment datasets, and convert files to 3D printable format.
“The unique advantage of image-based 3D printing is the ability to demonstrate anatomical spatial relationships with sub-millimeter accuracy. ”
”
Jeffrey D. Hirsch, MD
Associate Professor, Director of Public Radiology, Department of Diagnostic Radiology University of Maryland Medicine
Formlabs-printed anatomy models are already being used by several subspecialists in surgery, including but not limited to orthopedic, cardiothoracic, vascular surgery, oral and maxillofacial surgery, oncology, plastic and reconstructive surgery, urology and pediatrics. This handbook provides an overview of the steps that can be applied to any Digital Imaging and Communications in Medicine (DICOM) dataset, which is the standard format for storing images in any modern Image Archiving and Communication Systems (PACS)
WHAT YOU NEED FOR IN-HOUSE 3D PRINTING
CT or MRI scan and associated DICOM file
- Recommended slice thickness: 0.25mm-1.25mm2
Computer with imaging software for segmentation or using an outsourced segmentation service
Form 2 3D printer and resin, e. g.:
g.:
- Orthopedic white resin or OMFS
- Transparent polymer for cardiovascular or urological surgery
- SG Dental Resin for Surgical Guides (for approved applications only)
Form Wash and Form Cure for 3D post-processing (recommended for medical models)
Applications and benefits of 3D printed anatomical models medicine. Please consider your intended use, local regulations, medical imaging approvals, material specifications, biocompatibility requirements, protected medical information, and institutional standards before 3D printing or using anatomical models
Depending on your institution, anatomical models may be used for patient or pathological purposes:
- Preoperative planning and intraoperative reference models for surgeons
- Device calibration (e.g. mandibular plates) and surgical instrument design*
- Molds for implant material or prostheses*
- Teaching and simulation laboratories
- Patient Education and Enhanced Informed Consent
* May be regulated and/or require institutional approval
Numerous published case studies and ongoing efforts have demonstrated the potential of 3D printing in clinical settings. Public use cases include preoperative planning3, intraoperative use4, patient-centric instrument kits5, customized implants6, bone cement molds or polymethyl methacrylate (PMMA) implants8, prostheses9and trays
Public use cases include preoperative planning3, intraoperative use4, patient-centric instrument kits5, customized implants6, bone cement molds or polymethyl methacrylate (PMMA) implants8, prostheses9and trays
These use cases have demonstrated success in a variety of fields and surgical specialties, including orthopedic, cardiac, oral and maxillofacial (OMFS), vascular, neurological, cardiothoracic, musculoskeletal, plastic and reconstructive surgery, oncology, pediatrics, interventional radiology, etc.
“While I would like to think that my brain can reconstruct a 3D interpretation from a 2D CT scan, I was surprised by the relative inaccuracy of the approach I have been using for 20 years. 3D models are invaluable in planning, especially when using the daVinci robot.”
Dr. Ronald Hrebinko
Urologist and Associate Professor of Urology
University of Pittsburgh School of Medicine
3D printed models can also provide significant benefits for the education of residents, fellows and students10.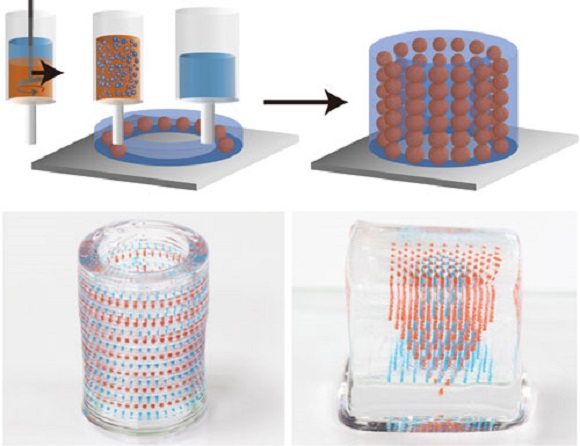 Individual models are particularly attractive when compared to the cost of cadaveric specimens and animal testing and the associated requirements for laboratory space, surgical instruments, and disposal
Individual models are particularly attractive when compared to the cost of cadaveric specimens and animal testing and the associated requirements for laboratory space, surgical instruments, and disposal
5 leading medical disciplines on the use of 3D printing technology
Chepelev et al.
Image sourced from http://www.materialise.com/en/blog/3d-printing-us-hospitals
Explore our collection of research publications, to learn more about how Formlabs printers and supplies are being used in healthcare.
The widespread use of advanced imaging in radiology has become a key factor in diagnosis and communication between physicians. While these visualizations have traditionally been used in the 2D plane as CT or MRI scans as DICOM files, software developers have recently created tools to reconstruct diagnostic images as 3D anatomical imaging.
3D printed models are a natural extension of these various 3D rendering options and offer many additional benefits such as tactile feedback and other tangible information that visualizations cannot provide.
When a patient's severe foot deformity could not be fully represented with 2D images, surgeons used a 3D printed model to plan how to correct gait with preoperative equipment and work with clinical staff and receptionists.
For example, research on a custom 3D printed model allowed a UK orthopedic surgeon to find a solution with a lower risk of abnormal injury to a boy's forearm
“Access to the model has changed standard CT-indicated therapy from a four-hour complex osteotomy to a simple, much less invasive 30-minute soft tissue procedure,” says Dr. Michael Eames
A successful operation was completed in just 30 minutes — reduction of more than three hours from the originally scheduled time in the operating room, saving the hospital an estimated $5,500. Subsequently, the patient spent less time on post-operative care and recovered more quickly
Workflows from scan to 3D model
Creating 3D printed files and 3D printed models requires special considerations and minor changes in the medical imaging workflow
The tailored workflow can be divided into three steps: image acquisition, image segmentation and 3D printing
IMAGE ACQUISITION
Image acquisition is the first step and is already integrated into the workflow. The most common imaging techniques suitable for 3D printing are CT and MRI. In general, 3D models can be printed from any volumetric image dataset (slices) with sufficient contrast to differentiate tissues.
The most common imaging techniques suitable for 3D printing are CT and MRI. In general, 3D models can be printed from any volumetric image dataset (slices) with sufficient contrast to differentiate tissues.
Cone-beam CT is also widely used for dental and otolaryngological imaging of teeth, but contrast can be worse than conventional CT, making segmentation more difficult. See recommendations for setting up patient scans for 3D models in Part 2 of this booklet. Once the radiographer has received the DICOM, they must perform Regions of Interest (ROI) processing, which will be rendered as a 3D printed object. The process of identifying and separating tissues and other areas of interest is called segmentation. Depending on the complexity of the model, it is performed by a radiologist-technician under the guidance of a radiologist or directly by a radiologist. Once the segmentation is completed, it is reviewed by the surgeon for final approval13
A number of commercial and open source software products can be used for the segmentation process (see the list at the end of this section).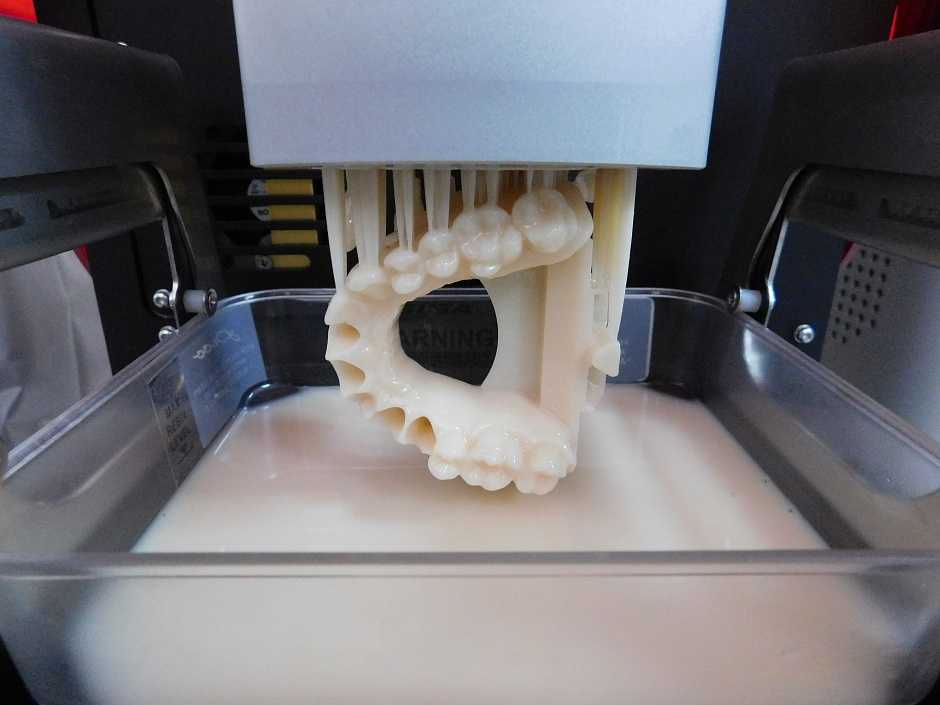 Before choosing a software solution, consider your intended use, regulatory requirements in your area, and recommendations at your institution.
Before choosing a software solution, consider your intended use, regulatory requirements in your area, and recommendations at your institution.
ROI segmentation steps can include automatic methods (eg thresholding, edge detection and region enlargement) or manual selection and adjustments. Thresholding uses parameters that can be identified and associated with a particular ROI, such as bones with higher Hounsfield values relative to their surroundings.
Thresholds may need to be dynamic and include more sophisticated algorithms to account for factors such as CT noise and beam hardening that can create artifacts and other unwanted results.
Another option is to use the growth region to automate segmentation, where the algorithm assigns voxels as belonging to one part or another based on similarity or difference to surrounding voxels. This may require additional adjustments and clarifications.
After segmentation is complete, convert the segmented objects to a file type that can be used by the 3D printer. This file type is usually an STL or OBJ file format.
This file type is usually an STL or OBJ file format.
After conversion, make any necessary physical adjustments that are more common in 3D modeling, such as smoothing surfaces, filling holes, and fixing other minor features. These adjustments can be made by a specialist in various CAD or CAM programs and should always include review by a physician to ensure that the result is clinically useful.
Once the radiologist has received DICOM, they must define regions of interest (ROIs) that will be displayed as a 3D printed object. Source: ITK-Snap
In-house 3D printing enables healthcare providers to quickly create high resolution medical models.
3D PRINT
Once the final file is ready, it can be exported and sent to the 3D printer for production. There are several key factors to consider when choosing the right 3D printing technology, including: the cost of the printer, software, and materials; print speed, accuracy and resolution; ease of use and access to customer service; the type of printed materials, including biocompatibility and sterilization for certain uses.
After printing, parts should be rinsed with isopropyl alcohol (IPA) to remove excess resin and, depending on the material and application, post-cured in a curing chamber. All biocompatible resins require post-cure prior to use, while standard Formlabs resins such as White and Clear Resin increase post-cure strength and stability.
Learn more about print options
Visit our Software Support and Resources pages for more information on how to set up files for printing and learn more about specifications such as internal supports and minimum wall thickness
POTENTIAL FIELD 3D PRINTING SOFTWARE AND HARDWARE
Note: Each section requires only one kind of software that completes the workflow steps. This list is for ease of reference and research and does not constitute an endorsement of any particular software or vendor. If you require anatomical models without segmentation or printing in situ, specialized service providers offer conversion, segmentation and/or printing services for a fee (e. g. Anatomage, Armor Bionics, Axial3D and Materialize)
g. Anatomage, Armor Bionics, Axial3D and Materialize)
Check your local regulations and intended use before choosing a software solution.
Transform + Segmentation
| Materialise Mimics* | ITK-SNAP |
| 3D Slicer | 4DICOM |
| Axial3D | Seg3D |
| Osirix | Embodi3D (DICOM - STL conversion, no segmentation) |
| Ossa 3D | Vitrea Vital Images |
| Anatomage Medical Design Studio |
Preparation for editing + File management, smoothing and identification
| Blender | Materialize 3matic | Autodesk Meshmixer |
Support Generation + Print Orientation
| Formlabs PreForm | Materialize e-Stage Note: Cardiac cases may require advanced removal of supports from within the valves (PreForm video tutorial) |
Printer
| Formlabs Form 2 or Form Cell system | Formlabs Fuse 1 |
Post-print
| Formlabs finishing kit | Form Wash and Form Cure 9029four |
Ultrasonic cleaner (e. g. GT Sonic) g. GT Sonic) | CUREBox CB-4051 |
* Formlabs and Materialize have partnered to offer a comprehensive package of services in the US, Europe and Japan. Mimics inPrint is a specialized software solution for creating accurate virtual anatomical models from medical images and preparing files for 3D printing. Integrated into Clinical Environments (PACS), Mimics inPrint includes predefined workflows with direct link to Formlabs 3D printers.
Patient Scan Setup for 3D Models
Some conventional medical imaging scans cannot be converted to high quality 3D models for clear and accurate anatomical structures. Plain radiographs (X-rays) and ultrasounds are not commonly used for 3D printing and these imaging techniques are not recommended.
The most commonly used imaging modalities for evaluating internal structures are computed tomography and MRI imaging. These rendering methods generate a DICOM file. DICOM is a standard for storing and transmitting medical images and can be thought of as a series of slices.
DICOM images cannot be edited in 3D design software or sent directly to a printer. To convert a DICOM file to a format suitable for 3D printing, such as an STL or OBJ file, separate software is required to calculate the surface area of interest. This surface will become a 3D model.
Almost any DICOM file with sufficiently fine detail (such as thin slices) can be converted to a format that supports 3D printing of the structure of interest.
The following articles may be helpful in preparing, printing and post-processing anatomy models:
Design models for print support
Design features and geometric recommendations
Post-curing printing
Post-processing basics
Criteria for creating a printable scan
The first consideration when converting a CT or MRI to a 3D model is what needs to be shown; bones, vessels, and whole organs are all modeled differently. A model with outdated structures not only detracts from the focus of the model, but it will also be harder to produce. Scanning at the right specifications makes it easy to create a 3D printable model. The main features are intravenous contrast and slice thickness.
A model with outdated structures not only detracts from the focus of the model, but it will also be harder to produce. Scanning at the right specifications makes it easy to create a 3D printable model. The main features are intravenous contrast and slice thickness.
For 3D models of bone structures, low contrast images are likely to be sufficient for accurate and detailed printing. Models containing solid organs, tumors, or vascular structures almost always require contrast magnification scans
Introductory contrast information
CT brightness variation allows the segmentation software to highlight different structures, allowing you to print an area or organ of interest. Some structures, such as bones, are inherently bright on CT scans. This makes it easier to 3D print when started from a non-contrast CT. However, intravenous
(IV) contrast is needed when you want to 3D print a blood vessel, tumor, or most organs. A contrast agent is injected into the patient just before the scan. With IV contrast, blood vessels (arteries and veins) and solid organs (such as the liver, kidneys, spleen, heart, and brain) become brighter when scanned, allowing the segmentation software to accurately separate them from surrounding tissues. See images below for a comparison of non-contrast and contrast-enhanced CT scans of the abdomen.
With IV contrast, blood vessels (arteries and veins) and solid organs (such as the liver, kidneys, spleen, heart, and brain) become brighter when scanned, allowing the segmentation software to accurately separate them from surrounding tissues. See images below for a comparison of non-contrast and contrast-enhanced CT scans of the abdomen.
The effect of intravenous contrast is shown with two axial (transverse) CT scans of the upper abdomen. On a right scan, the aorta is enhanced, whereas on a left scan, the aorta appears very similar to the adjacent soft tissue. The contrast allows you to isolate the desired structures in post-processing. Source: Embodi 3D
In addition to enhancing contrast, slice thickness and resolution are equally important for planning when creating a 3D model. Most clinically useful scans were obtained at adequate resolution for 3D printing. However, if you try to 3D print an anatomical model while scanning with thick sections, your
model will have a rough surface. According to numerous sources, when creating a model for 3D printing, it is very important to use scans with slices less than 1.25 mm.
According to numerous sources, when creating a model for 3D printing, it is very important to use scans with slices less than 1.25 mm.
Two CT scans of the chest. The image on the left shows a frontal view constructed from 5 mm thick slices, while the high resolution scan shows a similar view of the chest using only 1 mm thick slices. Thick slices in the left image create rough textures that will result in a lower quality print. Source: Embodi 3D
The thickness of sections obtained from CT or MRI scans are converted directly into details generated from 3D scans. Depending on the focus object, areas of the image should be reconstructed with isotropic voxels of 1.25 mm or less15. According to a Mayo Clinic presentation in March 2016, 1 to 5 mm slices can be used for large structures, while 0.75 mm can be used for thin bone16. Thicker regions may degrade model accuracy, while very thin regions (e.g. <0.25 mm) may require extensive segmentation and STL enhancement, especially in the presence of image artifact. Cardiac models show sufficient accuracy with 0.5 mm patches, but thinner targets may be required for thin objects such as the inferior wall of the orbit17. Generally, thicker areas can create fuzzy or less accurate prints. However, unnecessarily thin areas can lead to significantly more work in the post-processing step.
Cardiac models show sufficient accuracy with 0.5 mm patches, but thinner targets may be required for thin objects such as the inferior wall of the orbit17. Generally, thicker areas can create fuzzy or less accurate prints. However, unnecessarily thin areas can lead to significantly more work in the post-processing step.
Regulatory Issues
Please check local regulations, material data, patient information, and institutional requirements before 3D printing or using anatomical models. If you work in the US, please refer to the latest FDA presentation which outlines its guidance document18 Please note that these documents and recommendations are subject to change. Make sure you are using the latest guidelines.
Formlabs is the industry's leading manufacturer of 3D printers and materials used by healthcare providers to support the practice of medicine
Conclusion
Barriers to the transition to personalized precision medicine are fast disappearing. The advent of affordable, professional-grade 3D printers has enabled healthcare providers to produce anatomy models for specific patients and specialties with inspiring results. In some cases, the initial cost of a high quality printer has been covered by the time saved in the operating room after the surgeon used the 3D printed model to prepare for one complex procedure.19
The advent of affordable, professional-grade 3D printers has enabled healthcare providers to produce anatomy models for specific patients and specialties with inspiring results. In some cases, the initial cost of a high quality printer has been covered by the time saved in the operating room after the surgeon used the 3D printed model to prepare for one complex procedure.19
“Medicine is not a one-size-fits-all solution, and when a tool like desktop 3D printing comes along that allows you to create personalized medical solutions, there is no doubt that it needs to be used to its full potential.”
Todd Goldstein
Instructor, Institute for Medical Research. Feinstein Director, 3D Printing Lab, Northwell Ventures, Northwell Health
Understanding the workflow required to integrate 3D printing is key to success.
This tutorial covers everything you need to get started, popular workflows, and tools and techniques to ease the transition from patient scanning to 3D printing
Contact us to learn more about 3D printing in Your institution and join the community of innovators in precision medicine
REFERENCES
- Chepelev, Leonid, Andreas Giannopoulos, Anji Tan, Dimitrios Mitsouras and Frank J.
 Rybicki Medical 3D Printing: Terminology Standardization Techniques and Report Trends 3D- printing in medicine 3, no. 1 (2017) doi:101186/s41205-017-0012-5
Rybicki Medical 3D Printing: Terminology Standardization Techniques and Report Trends 3D- printing in medicine 3, no. 1 (2017) doi:101186/s41205-017-0012-5 - Mitsworth, Dimitris, Peter Lakouras, Amir Imanzadeh, Andreas A Giannopoulos, Tianrun Kai, Kanako K. Kumamaru, Elizabeth George, et al. "3D Medical Printing for the Radiologist" RadioGraphics 35, no. 7 (November 2015): 1965–88 https ://doi.org/101148/rg2015140320
- Kerr, William, Philip Rowe, and Steven Gareth Pierce "Accurate 3D Bone Reconstruction Using Ultrasonic Synthetic Aperture Techniques for Robotic Knee Arthroplasty" Computerized Medical Imaging and Graphics 58 (June 2017): 23–32 https://doi org/101016/j compmedimag 201703 002
- Chen, Xing, Jesse K Possel, Katherine Waconne, Ann F van Ham, P. Christian Klink, and Peter R. Roelfsema “3D printing and modeling of customized implants and surgical guides for lower primates” Journal of Neuroscience Methods 286 (July 2017) ): 38–55 https://doi org/101016/jjneumeth 201705 013
- Wong, K.
 S., S.M. Kumta, N. V. Geel and J. Demol "One-stage reconstruction with a 3D printed, biomechanically assessed custom implant after complex resection of pelvic tumors" Computer Surgery 20, no. 1 (January 2, 2015): 14–23 https:// doi org/10 3109/1092908820151076039
S., S.M. Kumta, N. V. Geel and J. Demol "One-stage reconstruction with a 3D printed, biomechanically assessed custom implant after complex resection of pelvic tumors" Computer Surgery 20, no. 1 (January 2, 2015): 14–23 https:// doi org/10 3109/1092908820151076039 - Tan, Eddie T.V., Ji Ming Lin, and Shri Kumar Dinesh “Creating Acrylic Patient Cranioplasty Implants with an Inexpensive 3D Printer” Journal of Neurosurgery 124, no. 5 (May 2016): 1531–37 https://doi org/10 3171/2015 5 jns15119
- Tan, Eddie T.V., Ji Ming Lin, and Shri Kumar Dinesh “Creating Acrylic Patient Cranioplasty Implants with an Inexpensive 3D Printer” Journal of Neurosurgery 124, no. 5 (May 2016): 1531–37 https://doi org/10 3171/2015 5 jns15119
- Abdel Hey, Joe, Tarek Smyra, and Ronald Moussa "Customized Implants with PMMA Cranioplasty Using 3D Polylactic Acid Printing Plates: Technical Note with 2 Illustrative Examples" World Neurosurgery 105 (September 2017): 971–979 e1 https http://doi.org/101016/j wneu 201705 00
- Keith, Jelleten, Gerwin Smith, and Paul Bredveld, 3D Printed Upper Limb Prosthesis: A Review of Disability and Rehabilitation: Rehabilitation Techniques 12, no.
 3 (February 2, 2017): 300–314 https://doi org/ 101080/1748310720161253117
3 (February 2, 2017): 300–314 https://doi org/ 101080/1748310720161253117 - Azer, Sami A., and Sarah Azer, “3D Anatomical Models and Impact on Learning: A Review of Quality in the Literature,” Health Professions Education 2, no. 2 (December 2016): 80–98 https://doi org/101016 /j hpe 2016 05 002
- Planning with a custom surgical model reduces OR time by 88 percent" Formlabs Accessed November 22, 2017 https://formlabs com/preoperative-planning-with-custom-3d-printed-surgical-model-reduces-theater-time/
- Christensen, Andy "Medical Imaging Software" 3D printing | Wohlers Associates Accessed November 22, 2017 http://www.wohlersassociates com/
- Matsumoto, Jane S., Jonathan M. Morris, Thomas Foley, Eric E. Williamson, Shuai Leng, Ciarán P McGay, Joel L. Kuhlmann, Linda E. Nesberg, and Terry J. Vrtiska 3D Physical Modeling: Applications and Experiences in Mayo Clinic RadioGraphics 35, No. 7 (2015): 1989-2006 doi:101148/rg 2015140260
- Kikinis R, Pieper SD, Vosburg K (2014) 3D Slicer: a platform for subject image analysis, visualization and clinical support.
 Intraoperative image processing. Imaging Therapy, Ferenc A. Jolez, Editor 3 (19): 277-289 ISBN : 978-1-4614-7656-6 (Print) 978-1-4614-7657-3 (Online) https://www slicerorg/wiki/ CitingSlicer
Intraoperative image processing. Imaging Therapy, Ferenc A. Jolez, Editor 3 (19): 277-289 ISBN : 978-1-4614-7656-6 (Print) 978-1-4614-7657-3 (Online) https://www slicerorg/wiki/ CitingSlicer - Mitsworth, Dimitris, Peter Lakouras, Amir Imanzadeh, Andreas A Giannopoulos, Tianrun Kai, Kanako K. Kumamaru, Elizabeth George, et al. "3D Medical Printing for the Radiologist" RadioGraphics 35, no. 7 (November 2015): 1965–88 https ://doi.org/101148/rg2015140320
- TJ Vrtiska, MD, Jane Matsumoto, MD, Jay Morris, MD, Imaging: The Role of the Radiologist. A Key First Step” Mayo Clinic (March 4, 2016)
- Mitsworth, Dimitris, Peter Lakouras, Amir Imanzadeh, Andreas A Giannopoulos, Tianrun Kai, Kanako K. Kumamaru, Elizabeth George, et al. "3D Medical Printing for the Radiologist" RadioGraphics 35, no. 7 (November 2015): 1965–88 https ://doi.org/101148/rg2015140320
- Nooshin Kiarashi, PhD, FDA/CDRH/Department of Radiological Medicine, "FDA Current Practice and Regulations, FDA/CDRH-RSNA SIG Joint Meeting on Customized 3D Printed Anatomical Models", excerpted from https://www fda gov/ downloads/MedicalDevices/NewsEvents/WorkshopsConferences/ UCM575723 pdf
- Preoperative-planning-with-custom-3d-printed-surgical-model-reduces-theater-time by 88 percent Formlabs Accessed November 22, 2017
ADDITIONAL RESOURCES AND LINKS
1531–37 https://doi org/10 3171/2015 5 jns15119 Kikinis R. , Pieper S.D., Vosburg K. (2014) 3D Slicer: a platform for object-based image analysis , imaging and clinical support. Intraoperative image processing. Imaging Therapy, Ferenc A. Jolez, Editor 3 (19): 277-289 ISBN : 978-1-4614-7656-6 (Print) 978-1-4614-7657-3 (Online)
, Pieper S.D., Vosburg K. (2014) 3D Slicer: a platform for object-based image analysis , imaging and clinical support. Intraoperative image processing. Imaging Therapy, Ferenc A. Jolez, Editor 3 (19): 277-289 ISBN : 978-1-4614-7656-6 (Print) 978-1-4614-7657-3 (Online)
Rybicki F. Christensen, A. (05/12/2017) Recommendations for Medical 3D print: Patient safety. Retrieved Nov 03, 2017 from https://www 3printrcom/ guidelines-medical-3d-printing-patient- safety-3345869/ (n d ) http://www conceptualiz com/resources html
Biomedical Modeling, Inc Materials (16.10 .2013) Biomodeling process: From 2D to 3D https://www slideshare net/Biomedical_Modeling_Inc/the- biomodeling-process-from-2d-to-3d-27259255
Choosing the Best Medical Imaging Scan for 3D Printed Medical Models (December 27, 2016) https://www embodi3d com/blogs/entry/183-choosing-the-best-medical-imaging-scan-to- create-a-3d-printed-medical-model/
Documentation/4 6/Training (n d ) https://www slicerorg/wiki/ Documentation/4.