Ct scan to 3d print
3D printing from cardiovascular CT: a practical guide and review
1. Lee JW, Lee G, Lee NK, et al. Effectiveness of Adaptive Statistical Iterative Reconstruction for 64-Slice Dual-Energy Computed Tomography Pulmonary Angiography in Patients With a Reduced Iodine Load: Comparison With Standard Computed Tomography Pulmonary Angiography. J Comput Assist Tomogr 2016;40:777-83. 10.1097/RCT.0000000000000443 [PubMed] [CrossRef] [Google Scholar]
2. Ryu YJ, Choi YH, Cheon JE, et al. Knowledge-based iterative model reconstruction: comparative image quality and radiation dose with a pediatric computed tomography phantom. Pediatr Radiol 2016;46:303-15. 10.1007/s00247-015-3486-6 [PubMed] [CrossRef] [Google Scholar]
3. Otton JM, Kühl JT, Kofoed KF, et al. Four-dimensional image processing of myocardial CT perfusion for improved image quality and noise reduction. J Cardiovasc Comput Tomogr 2013;7:110-6. 10.1016/j.jcct.2013.01.014 [PubMed] [CrossRef] [Google Scholar]
4. Nishii T, Kono AK, Tani W, et al. Four-dimensional noise reduction using the time series of medical computed tomography datasets with short interval times: a static-phantom study. PeerJ 2016;4:e1680. 10.7717/peerj.1680 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
5. Tandon A, Byrne N, Nieves Velasco Forte Mde L, et al. Use of a semi-automated cardiac segmentation tool improves reproducibility and speed of segmentation of contaminated right heart magnetic resonance angiography. Int J Cardiovasc Imaging 2016;32:1273-9. 10.1007/s10554-016-0906-0 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
6. Withey DJ, Koles ZJ. A review of medical image segmentation: methods and available software. International Journal of Bioelectromagnetism 2008;10:125-48. [Google Scholar]
7. Byrne N, Velasco Forte M, Tandon A, et al. A systematic review of image segmentation methodology, used in the additive manufacture of patient-specific 3D printed models of the cardiovascular system. JRSM Cardiovasc Dis 2016;5:2048004016645467. 10.1177/2048004016645467 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
10.1177/2048004016645467 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
8. Greil GF, Kuettner A, Flohr T, et al. High-resolution reconstruction of a waxed heart specimen with flat panel volume computed tomography and rapid prototyping. J Comput Assist Tomogr 2007;31:444-8. 10.1097/01.rct.0000238012.49684.69 [PubMed] [CrossRef] [Google Scholar]
9. Farooqi KM, Lengua CG, Weinberg AD, et al. Blood Pool Segmentation Results in Superior Virtual Cardiac Models than Myocardial Segmentation for 3D Printing. Pediatr Cardiol 2016;37:1028-36. 10.1007/s00246-016-1385-8 [PubMed] [CrossRef] [Google Scholar]
10. Greil GF, Wolf I, Kuettner A, et al. Stereolithographic reproduction of complex cardiac morphology based on high spatial resolution imaging. Clin Res Cardiol 2007;96:176-85. 10.1007/s00392-007-0482-3 [PubMed] [CrossRef] [Google Scholar]
11. Park EK, Lim JY, Yun IS, et al. Cranioplasty Enhanced by Three-Dimensional Printing: Custom-Made Three-Dimensional-Printed Titanium Implants for Skull Defects. J Craniofac Surg 2016;27:943-9. 10.1097/SCS.0000000000002656 [PubMed] [CrossRef] [Google Scholar]
J Craniofac Surg 2016;27:943-9. 10.1097/SCS.0000000000002656 [PubMed] [CrossRef] [Google Scholar]
12. Schmauss D, Haeberle S, Hagl C, et al. Three-dimensional printing in cardiac surgery and interventional cardiology: a single-centre experience. Eur J Cardiothorac Surg 2015;47:1044-52. 10.1093/ejcts/ezu310 [PubMed] [CrossRef] [Google Scholar]
13. Shi D, Liu K, Zhang X, et al. Applications of three-dimensional printing technology in the cardiovascular field. Intern Emerg Med 2015;10:769-80. 10.1007/s11739-015-1282-9 [PubMed] [CrossRef] [Google Scholar]
14. Rengier F, Mehndiratta A, von Tengg-Kobligk H, et al. 3D printing based on imaging data: review of medical applications. Int J Comput Assist Radiol Surg 2010;5:335-41. 10.1007/s11548-010-0476-x [PubMed] [CrossRef] [Google Scholar]
15. Matsumoto JS, Morris JM, Foley TA, et al. Three-dimensional Physical Modeling: Applications and Experience at Mayo Clinic. Radiographics 2015;35:1989-2006. 10.1148/rg.2015140260 [PubMed] [CrossRef] [Google Scholar]
16. Mitsouras D, Liacouras P, Imanzadeh A, et al. Medical 3D Printing for the Radiologist. Radiographics 2015;35:1965-88. 10.1148/rg.2015140320 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
Mitsouras D, Liacouras P, Imanzadeh A, et al. Medical 3D Printing for the Radiologist. Radiographics 2015;35:1965-88. 10.1148/rg.2015140320 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
17. Gómez-Ciriza G, Hussain T, Gómez-Cía T, et al. Potential of 3D-printed models in planning structural interventional procedures. Interventional Cardiology 2015;7:345-52. 10.2217/ica.15.25 [CrossRef] [Google Scholar]
18. O'Reilly MK, Reese S, Herlihy T, et al. Fabrication and assessment of 3D printed anatomical models of the lower limb for anatomical teaching and femoral vessel access training in medicine. Anat Sci Educ 2016;9:71-9. 10.1002/ase.1538 [PubMed] [CrossRef] [Google Scholar]
19. Lim KH, Loo ZY, Goldie SJ, et al. Use of 3D printed models in medical education: A randomized control trial comparing 3D prints versus cadaveric materials for learning external cardiac anatomy. Anat Sci Educ 2016;9:213-21. 10.1002/ase.1573 [PubMed] [CrossRef] [Google Scholar]
20. McMenamin PG, Quayle MR, McHenry CR, et al. The production of anatomical teaching resources using three-dimensional (3D) printing technology. Anat Sci Educ 2014;7:479-86. 10.1002/ase.1475 [PubMed] [CrossRef] [Google Scholar]
The production of anatomical teaching resources using three-dimensional (3D) printing technology. Anat Sci Educ 2014;7:479-86. 10.1002/ase.1475 [PubMed] [CrossRef] [Google Scholar]
21. AbouHashem Y, Dayal M, Savanah S, et al. The application of 3D printing in anatomy education. Med Educ Online 2015;20:29847 10.3402/meo.v20.29847 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
22. Reuthebuch O, Lang A, Groscurth P, et al. Advanced training model for beating heart coronary artery surgery: the Zurich heart-trainer. Eur J Cardiothorac Surg 2002;22:244-8. 10.1016/S1010-7940(02)00269-5 [PubMed] [CrossRef] [Google Scholar]
23. Deferm S, Meyns B, Vlasselaers D, et al. 3D-Printing in Congenital Cardiology: From Flatland to Spaceland. J Clin Imaging Sci 2016;6:8. 10.4103/2156-7514.179408 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
24. Biglino G, Capelli C, Wray J, et al. 3D-manufactured patient-specific models of congenital heart defects for communication in clinical practice: feasibility and acceptability.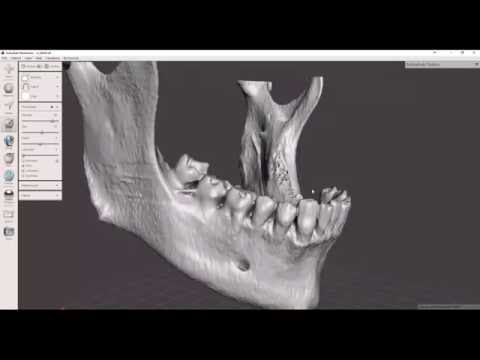 BMJ Open 2015;5:e007165. 10.1136/bmjopen-2014-007165 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
BMJ Open 2015;5:e007165. 10.1136/bmjopen-2014-007165 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
25. Loke T, Krieger A, Sable C, et al. Novel Uses for Three-Dimensional Printing in Congenital Heart Disease. Current Pediatrics Reports 2016;4:28-34. 10.1007/s40124-016-0099-y [CrossRef] [Google Scholar]
26. Health NIo. NIH 3D print exchange. 2014. Available online: https://3dprint.nih.gov/
27. Ngan EM, Rebeyka IM, Ross DB, et al. The rapid prototyping of anatomic models in pulmonary atresia. J Thorac Cardiovasc Surg 2006;132:264-9. 10.1016/j.jtcvs.2006.02.047 [PubMed] [CrossRef] [Google Scholar]
28. Noecker AM, Chen JF, Zhou Q, et al. Development of patient-specific three-dimensional pediatric cardiac models. ASAIO J 2006;52:349-53. 10.1097/01.mat.0000217962.98619.ab [PubMed] [CrossRef] [Google Scholar]
29. Sodian R, Weber S, Markert M, et al. Stereolithographic models for surgical planning in congenital heart surgery. Ann Thorac Surg 2007;83:1854-7. 10.1016/j.athoracsur.2006.12.004 [PubMed] [CrossRef] [Google Scholar]
10.1016/j.athoracsur.2006.12.004 [PubMed] [CrossRef] [Google Scholar]
30. Sodian R, Weber S, Markert M, et al. Pediatric cardiac transplantation: three-dimensional printing of anatomic models for surgical planning of heart transplantation in patients with univentricular heart. J Thorac Cardiovasc Surg 2008;136:1098-9. 10.1016/j.jtcvs.2008.03.055 [PubMed] [CrossRef] [Google Scholar]
31. Vranicar M, Gregory W, Douglas WI, et al. The use of stereolithographic hand held models for evaluation of congenital anomalies of the great arteries. Stud Health Technol Inform 2008;132:538-43. [PubMed] [Google Scholar]
32. Shiraishi I, Yamagishi M, Hamaoka K, et al. Simulative operation on congenital heart disease using rubber-like urethane stereolithographic biomodels based on 3D datasets of multislice computed tomography. Eur J Cardiothorac Surg 2010;37:302-6. [PubMed] [Google Scholar]
33. Jacobs S, Grunert R, Mohr FW, Falk V. 3D-Imaging of cardiac structures using 3D heart models for planning in heart surgery: a preliminary study. Interact Cardiovasc Thorac Surg 2008;7:6-9. 10.1510/icvts.2007.156588 [PubMed] [CrossRef] [Google Scholar]
Interact Cardiovasc Thorac Surg 2008;7:6-9. 10.1510/icvts.2007.156588 [PubMed] [CrossRef] [Google Scholar]
34. Sodian R, Schmauss D, Markert M, et al. Three-dimensional printing creates models for surgical planning of aortic valve replacement after previous coronary bypass grafting. Ann Thorac Surg 2008;85:2105-8. 10.1016/j.athoracsur.2007.12.033 [PubMed] [CrossRef] [Google Scholar]
35. Schmauss D, Gerber N, Sodian R. Three-dimensional printing of models for surgical planning in patients with primary cardiac tumors. J Thorac Cardiovasc Surg 2013;145:1407-8. 10.1016/j.jtcvs.2012.12.030 [PubMed] [CrossRef] [Google Scholar]
36. Schmauss D, Juchem G, Weber S, et al. Three-dimensional printing for perioperative planning of complex aortic arch surgery. Ann Thorac Surg 2014;97:2160-3. 10.1016/j.athoracsur.2014.02.011 [PubMed] [CrossRef] [Google Scholar]
37. Son KH, Kim KW, Ahn CB, et al. Surgical Planning by 3D Printing for Primary Cardiac Schwannoma Resection. Yonsei Med J 2015;56:1735-7. 10.3349/ymj.2015.56.6.1735 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
10.3349/ymj.2015.56.6.1735 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
38. Shirakawa T, Koyama Y, Mizoguchi H, et al. Morphological analysis and preoperative simulation of a double-chambered right ventricle using 3-dimensional printing technology. Interact Cardiovasc Thorac Surg 2016;22:688-90. 10.1093/icvts/ivw009 [PubMed] [CrossRef] [Google Scholar]
39. Sørensen TS, Greil GF, Hansen OK, et al. Surgical simulation--a new tool to evaluate surgical incisions in congenital heart disease? Interact Cardiovasc Thorac Surg 2006;5:536-9. 10.1510/icvts.2006.132316 [PubMed] [CrossRef] [Google Scholar]
40. Sørensen TS, Mosegaard J, Greil GF, et al. Images in cardiovascular medicine. Virtual cardiotomy for preoperative planning. Circulation 2007;115:e312. 10.1161/CIRCULATIONAHA.106.667618 [PubMed] [CrossRef] [Google Scholar]
41. Sørensen TS, Beerbaum P, Mosegaard J, et al. Virtual cardiotomy based on 3-D MRI for preoperative planning in congenital heart disease. Pediatr Radiol 2008;38:1314-22. 10.1007/s00247-008-1032-5 [PubMed] [CrossRef] [Google Scholar]
Pediatr Radiol 2008;38:1314-22. 10.1007/s00247-008-1032-5 [PubMed] [CrossRef] [Google Scholar]
42. Vaquerizo B, Theriault-Lauzier P, Piazza N. Percutaneous Transcatheter Mitral Valve Replacement: Patient-specific Three-dimensional Computer-based Heart Model and Prototyping. Rev Esp Cardiol (Engl Ed) 2015;68:1165-73. 10.1016/j.rec.2015.08.005 [PubMed] [CrossRef] [Google Scholar]
43. Ripley B, Kelil T, Cheezum MK, et al. 3D printing based on cardiac CT assists anatomic visualization prior to transcatheter aortic valve replacement. J Cardiovasc Comput Tomogr 2016;10:28-36. 10.1016/j.jcct.2015.12.004 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
44. Dankowski R, Baszko A, Sutherland M, et al. 3D heart model printing for preparation of percutaneous structural interventions: description of the technology and case report. Kardiol Pol 2014;72:546-51. 10.5603/KP.2014.0119 [PubMed] [CrossRef] [Google Scholar]
45. Schmauss D, Schmitz C, Bigdeli AK, et al. Three-dimensional printing of models for preoperative planning and simulation of transcatheter valve replacement.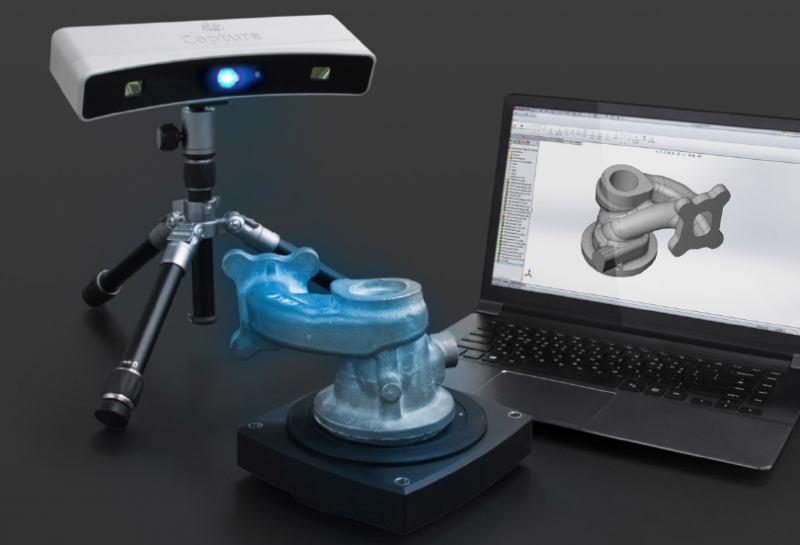 Ann Thorac Surg 2012;93:e31-3. 10.1016/j.athoracsur.2011.09.031 [PubMed] [CrossRef] [Google Scholar]
Ann Thorac Surg 2012;93:e31-3. 10.1016/j.athoracsur.2011.09.031 [PubMed] [CrossRef] [Google Scholar]
46. Otton JM, Spina R, Sulas R, et al. Left Atrial Appendage Closure Guided by Personalized 3D-Printed Cardiac Reconstruction. JACC Cardiovasc Interv 2015;8:1004-6. 10.1016/j.jcin.2015.03.015 [PubMed] [CrossRef] [Google Scholar]
47. Bartel T, Rivard A, Jimenez A, et al. Three-dimensional printing for quality management in device closure of interatrial communications. Eur Heart J Cardiovasc Imaging 2016;17:1069. 10.1093/ehjci/jew119 [PubMed] [CrossRef] [Google Scholar]
48. Chaowu Y, Hua L, Xin S. Three-Dimensional Printing as an Aid in Transcatheter Closure of Secundum Atrial Septal Defect With Rim Deficiency: In Vitro Trial Occlusion Based on a Personalized Heart Model. Circulation 2016;133:e608-10. 10.1161/CIRCULATIONAHA.115.020735 [PubMed] [CrossRef] [Google Scholar]
49. Kim MS, Hansgen AR, Wink O, et al. Rapid prototyping: a new tool in understanding and treating structural heart disease. Circulation 2008;117:2388-94. 10.1161/CIRCULATIONAHA.107.740977 [PubMed] [CrossRef] [Google Scholar]
Circulation 2008;117:2388-94. 10.1161/CIRCULATIONAHA.107.740977 [PubMed] [CrossRef] [Google Scholar]
50. Sodian R, Schmauss D, Schmitz C, et al. 3-dimensional printing of models to create custom-made devices for coil embolization of an anastomotic leak after aortic arch replacement. Ann Thorac Surg 2009;88:974-8. 10.1016/j.athoracsur.2009.03.014 [PubMed] [CrossRef] [Google Scholar]
51. Ibrahim D, Broilo TL, Heitz C, et al. Dimensional error of selective laser sintering, three-dimensional printing and PolyJet models in the reproduction of mandibular anatomy. J Craniomaxillofac Surg 2009;37:167-73. 10.1016/j.jcms.2008.10.008 [PubMed] [CrossRef] [Google Scholar]
52. Taft RM, Kondor S, Grant GT. Accuracy of rapid prototype models for head and neck reconstruction. J Prosthet Dent 2011;106:399-408. 10.1016/S0022-3913(11)60154-6 [PubMed] [CrossRef] [Google Scholar]
53. Choi JY, Choi JH, Kim NK, et al. Analysis of errors in medical rapid prototyping models. Int J Oral Maxillofac Surg 2002;31:23-32. 10.1054/ijom.2000.0135 [PubMed] [CrossRef] [Google Scholar]
10.1054/ijom.2000.0135 [PubMed] [CrossRef] [Google Scholar]
54. Hazeveld A, Huddleston Slater JJ, Ren Y. Accuracy and reproducibility of dental replica models reconstructed by different rapid prototyping techniques. Am J Orthod Dentofacial Orthop 2014;145:108-15. 10.1016/j.ajodo.2013.05.011 [PubMed] [CrossRef] [Google Scholar]
55. Hockaday LA, Kang KH, Colangelo NW, et al. Rapid 3D printing of anatomically accurate and mechanically heterogeneous aortic valve hydrogel scaffolds. Biofabrication 2012;4:035005. 10.1088/1758-5082/4/3/035005 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
56. Ma X, Qu X, Zhu W, et al. Deterministically patterned biomimetic human iPSC-derived hepatic model via rapid 3D bioprinting. Proc Natl Acad Sci U S A 2016;113:2206-11. 10.1073/pnas.1524510113 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
57. Cheung DY, Duan B, Butcher JT. Current progress in tissue engineering of heart valves: multiscale problems, multiscale solutions. Expert Opin Biol Ther 2015;15:1155-72. 10.1517/14712598.2015.1051527 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
Expert Opin Biol Ther 2015;15:1155-72. 10.1517/14712598.2015.1051527 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
58. Mosadegh B, Xiong G, Dunham S, et al. Current progress in 3D printing for cardiovascular tissue engineering. Biomed Mater 2015;10:034002. 10.1088/1748-6041/10/3/034002 [PubMed] [CrossRef] [Google Scholar]
Combine CT Scanning with Additive Manufacturing
In the medical field, computed tomography (CT) scanning has helped enable new 3D printing applications—physicians can use 3D-printed models of human organs (like the heart) generated from highly accurate CT scans of patients to prepare for complex surgeries, for example.
However, CT scanners could play an even more important role in additive manufacturing in the future by providing detailed quality scans of printed parts for many industries. They are already being used to scan items for reverse engineering operations that use 3D printing.
“3D printing allows you to produce previously impossible products, but you cannot inspect them without 3D scanning,” says Gerd Schwaderer, business development, metrology, at Volume Graphics. “If you can’t inspect your product, you can’t sell it.”
“If you can’t inspect your product, you can’t sell it.”
“When it comes to 3D printing, it’s like somebody invented a problem that we already had the solution for.”
— Gerd Schwaderer, Volume Graphics
The CT scanner market is poised to reach $6.5 billion by 2022, according to a Transparency Market Research report. Unlike other types of 3D scanning and metrology, CT scanners can provide precise dimensions of internal and external structures. The only other way to take those measurements is through destructive testing; you’d have to break the part or assembly to see inside.
Because 3D printing allows companies to produce parts with highly complex internal structures (channels or lattice patterns, for example), CT scanners can potentially help verify the accuracy of printed parts that are to be used in production environments. “We see a lot of interest in printing components because of the complexity it allows, particularly in aerospace and other industries,” says Steve Pilz, additive manufacturing product manager at ANSYS. “But there’s also this innate fear of putting one of these things on a plane or into production because they can’t see what’s inside.”
“But there’s also this innate fear of putting one of these things on a plane or into production because they can’t see what’s inside.”
As more additively manufactured parts are evaluated for use in critical applications (like aerospace or automotive) where accuracy and structural integrity are important, CT can take those measurements without destroying costly parts.
“CT scanning is really the natural companion of 3D printing,” Schwaderer says. “When it comes to 3D printing, it’s like somebody invented a problem that we already had the solution for.”
For polymers, CT scanning can detect potential part failures. “I can look at material flow and detect flaws in the manufacturing process that can’t otherwise be predicted,” says Rus Emerick, director of application engineering at Laser Design. “You can verify mold flow using CT and do a lot of fine-tuning.”
But so far there aren’t that many companies combining CT scans and 3D printing. In part, that’s because many customers don’t understand the technology or how it can benefit 3D print operations.
“They often have no clue how it works,” Schwaderer says. “They think it’s magic because they’ve only seen it in the context of a doctor’s office.”
CT scanning works by taking hundreds of X-ray images of a part as it is rotated inside the scanner. The 2D images are then combined to create a 3D point cloud. In quality applications, the CT image can then be compared to the CAD file to measure accuracy of the print.
“People don’t seem to understand they are two sides of the same coin,” says Giles Gaskell, applications manager at Wenzel America. “If you can make it on a 3D printer, you can measure it with a 3D scanner. If you are going to use 3D printing to make a part and it has a lot of internal detail, then you can’t measure it any other way.”
A printed object can be CT scanned, and the images can be passed through Simpleware software and into ANSYS’ software so designers can compare the physical object to the original CAD file.
Images courtesy of Synopsys.
Gaskell also theorizes that the reason many companies aren’t using CT scanning for quality inspection is that they aren’t really taking full advantage of 3D print capabilities. “If they were making full use of the technology, they’d be making parts that they couldn’t measure conventionally,” Gaskell says.
CT scanning has also improved significantly in resolution and speed over the past several years, while dropping in price. Many scanners can provide resolutions down to 5 to 7 microns (or less). The software running the scanner has also gotten easier to use, although interpreting scan results is still complex.
“CT is more of an interpretive science,” Emerick says. “To determine the edge of an object, if you are using laser scanners, then the edge is either there or it’s not. With CT analysis software you have to establish where the edge of the part really is, which is somewhere between air and 100% material. It takes some skill to interpret that data at the sub-voxel level. ”
”
Cost is also an issue. Although prices have fallen, quality CT scanners still cost hundreds of thousands of dollars. For many companies, outsourcing to a service provider is more cost effective.
Uncovering Inconsistency in 3D Printing
According to several sources contacted for this story, some 3D printer manufacturers and service providers have also pushed back against CT scanning because there are still significant quality issues with many 3D print processes. The accuracy of a print for the same part on two different machines, or on the same machine at different times or run by different operators, can vary significantly. Many printers still don’t provide the type of reliability and consistency required for mission-critical parts and components because of issues with porosity or delamination.
Porosity Zone indicates porosity within a 3D printed metal part along with varying density in the various layers along with visible voids. Image courtesy of Synopsys.
Image courtesy of Synopsys.
“There’s not only less interest among 3D printing people in CT; there’s a thinly disguised hostility in some cases,” Gaskell says. He describes an experience in which his company was given printed parts by a customer to evaluate against a CAD file. “We had a conference with the customer and printing people, and I thought the parts were being measured against the wrong CAD file,” Gaskell says. “The internal features had been so butchered by the printing process that they didn’t match the CAD anymore.”
Emerick agrees that CT scanning is critical for some 3D printing applications.
“The ugly truth is that additive manufacturing inherently causes flaws,” Emerick says. “With aerospace, if you get the slightest amount of porosity in the wrong place, you will break that part when you put [it] under a load. The more advanced companies realize they have to be able to analyze the quality and integrity of printed parts, but it’s still in the early stages. If it’s a mission-critical part, you should have a CT system to verify the structural integrity of the parts you are producing.”
If it’s a mission-critical part, you should have a CT system to verify the structural integrity of the parts you are producing.”
Deviations are a comparative analysis between CAD and the 3D printed specimen. Image courtesy of Synopsys.
He expects that as quality standards emerge and end users get a better grasp of 3D printing, there will be greater use of this type of CT scanning.
CT Scanning Limitations
3D printing doesn’t pose any special challenges when it comes to CT scans, but the inherent limitations of the scanning technology still apply.
Multi-material items are challenging, for example. This is particularly true if both metals and polymers are present. “You have to jack the power up to get through the metal, which overexposes the polymer,” Emerick says. “You may have to do multiple scans of the same assembly at different power settings to get a good final image.”
Dense materials might be difficult or impossible to scan. This is an important limitation in some aerospace and automotive applications where different types of metals are present. Titanium, for example, can be scanned but materials like cobalt chrome (which is used in high-heat applications) cannot.
This is an important limitation in some aerospace and automotive applications where different types of metals are present. Titanium, for example, can be scanned but materials like cobalt chrome (which is used in high-heat applications) cannot.
“The holy grail is to be able to 3D print turbine engine components with a lot of internal features rather than cast them,” Gaskell says. “CT struggles with that because the material is very dense, and that problem applies whether those are cast or printed parts. There’s not a machine powerful enough to scan the blades that is also accurate enough for the metrology on the inside of the part.”
“The closer you get to lead on the periodic table, the harder it will be,” Emerick adds. “Platinums, gold and silver cause a lot of problems. Inconel is [a] very noisy metal. Bronze is atrocious. Most people don’t understand metallurgy and the effect of irradiating metals, and how that impacts the quality of the scan.”
In addition, the size, geometry or thickness of the part can create scanning challenges. Printing materials may also display different behaviors than similar material used for casting. “We’ve run into that with additively manufactured parts,” says Nick Brinkhoff, product manager at North Star Imaging. “They tend to scatter differently than conventional parts.”
Printing materials may also display different behaviors than similar material used for casting. “We’ve run into that with additively manufactured parts,” says Nick Brinkhoff, product manager at North Star Imaging. “They tend to scatter differently than conventional parts.”
Quality Will Drive CT Adoption
The adoption of 3D printing is still in its nascent stages when it comes to end products and production parts. End users and printer manufacturers are still working to create consistency in additive manufacturing processes, develop quality standards and improve the handling and storage of sensitive materials.
And many companies aren’t yet designing for 3D printing—they are simply printing parts that could be cast or molded. Once the designs increase in complexity, the need for better measuring and inspection approaches will increase.
Gaskell expects that customers will eventually push for greater use of CT scanning for quality control and validation as they take advantage of 3D printing capabilities. CT scanners currently offer greater resolution than 3D printers, which means they are tailor made for identifying defects.
CT scanners currently offer greater resolution than 3D printers, which means they are tailor made for identifying defects.
The Wenzel exaCT U desktop CT solution can be customized for different applications. Image courtesy of Synopsys.
“CT is way ahead in terms of resolution,” Gaskell says. “When it comes to materials, the 3D printing people are ahead of us. They can print parts we can’t measure because of the material, but they can’t make parts that are more accurate than we can measure.”
Schwaderer thinks there could eventually be combined print and CT scan systems that do in-line inspection of builds as they are being made. “You could evaluate a print line by line because the printers operate so slowly,” Schwaderer says. “That would allow you to adjust the machine during the build, or stop a bad print early and start over.”
The key will be tying CT scans into CAD and simulation processes. CT scan data has to be converted into different file types to be useful to engineers.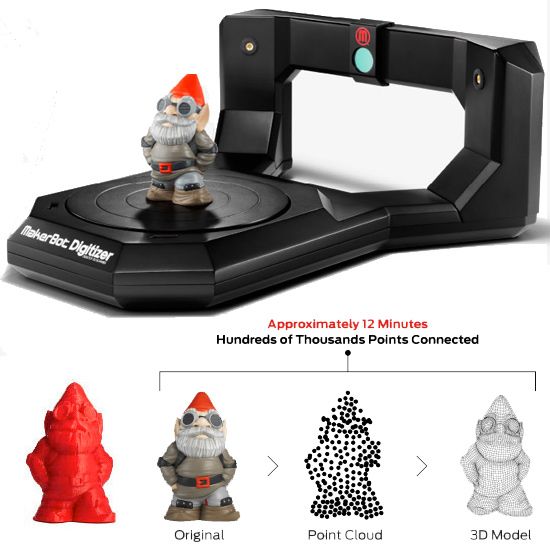 In some cases, the converted files may be too large to open in certain software programs.
In some cases, the converted files may be too large to open in certain software programs.
Volume Graphics has released a new Structural Mechanics Simulation Module for its VGSTUDIO MAX 3.0 that can take a CT file and (without meshing) calculate its porosity and do a simulation to determine if it is “good enough” for its application, even if there are imperfections.
By feeding CT scan information back into simulation tools, users can also create digital twins and simulate the performance of a physical part rather than a CAD file. ANSYS, North Star Imaging, and middleware provider Synopsys have done just that, in fact.
In 2016, Synopsys acquired Simpleware, which offers a solution that uses image-based meshing to convert CT scan images into files that can be used in finite element analysis tools. North Star can scan a printed object, then pass the images through Simpleware and into ANSYS’ systems so that designers can compare the physical object to the original CAD file, as well as run simulations based on the actual printed product.
“The key to this is high-value parts,” says Kerim Genc, Simpleware solution account manager at Synopsys. “You aren’t going to do this type of analysis on a cheap plastic part. Down the line, when you want to do scheduled maintenance on a high-value part and see how it is performing, you can also use CT scanning and FE models to do analysis. This isn’t just for the production line.”
Once the data is available, though, it can drive improvements across an organization. “We have customers who are trying to replace CMMs, and CT scanning gives them all the data they need for validation,” says Brinkhoff at North Star Imaging. “With one CT scan, you can do analysis for voids, do the dimensional inspection and run simulations.”
According to Emerick, CT is only going to increase in value for 3D printing and other types of manufacturing, because it provides a central set of data that can be used across multiple operations. “All the data is there,” Emerick says. “From metrology to porosity to stress.![]() You can do a complete structural stress analysis on the information provided, and everyone from engineering to manufacturing to marketing can extract the information they need. That’s a big deal.”
You can do a complete structural stress analysis on the information provided, and everyone from engineering to manufacturing to marketing can extract the information they need. That’s a big deal.”
More Info
ANSYS
GE Global Research
Laser Design
North Star Imaging
Synopsys
Transparency Market Research
Volume Graphics
Wenzel America
3D printing based on CT and MRI. Preoperative models
In our company you can order an urgent creation of high polygonal 3D models based on medical research. Data from MRI or CT images can be used as a base. The service is the digitization of a physical object, or the conversion of CT data for further modeling and printing of the model.
Range of services
- 3D modeling;
- 3D printing;
- Create a layout based on CT or MRI data.
Applications
Physical models that have been created on the basis of MRI or CT data are used very widely, allowing you to effectively solve various problems.
- Preparing for the operation – planning the operation is a complex and important process. With the help of models, specialists can work out the technique of the operation, select the tools, and clearly plan the course of the operation. As a result, the risks and time of surgery can be significantly reduced.
- Surgery - with the help of a printed model, you can assess the real state of affairs, accurately diagnose and build a treatment strategy, choose the optimal operational tactics, predict the consequences of injuries, etc.
- Dentistry - using data from CT or MRI images, 3D scanning and 3D printing, you can get high-quality models that will most accurately repeat all the anatomical features of the patient. Thus, dentistry can be brought to production capacity, eliminating errors and individualizing the results as much as possible. 3D printing and 3D modeling in the dental industry will help:
- store patient data in digital form;
- eliminate errors and reduce risks;
- increase volumes without increasing staff;
- to ensure the highest accuracy.

Dentists can use 3D modeling and 3D printing to make impressions, bite checks, make dentures and crowns, try them on, make orthodontic appliances. In addition, high-precision surgical templates can be made, which will allow high-precision placement of dental implants. As a result, the possibility of tissue damage is excluded, the risk of complications is reduced, the operation is facilitated, and the time of the intervention is also reduced.
With complex prosthetics, 3D scanning and 3D modeling, and subsequently 3D printing, can effectively solve even the most difficult clinical problems. All individual features will be taken into account, and therefore the prostheses will be as comfortable and safe as possible to wear.
- Cranioplasty is the restoration of the integrity of the skull, the elimination of defects (depressions, perforations, etc.) that have arisen for various reasons (congenital defects, gunshot wounds, decompression injuries, fractures, etc.
 ). The main indication for cranioplasty is the sealing of the tissues of the skull. For this purpose, various transplants (xeno-, allo-, autotransplants) are used. Based on CT and MRI data, it is possible to obtain accurate models that allow modeling an endoprosthesis or implant of the required shape and size in accordance with the missing part of the skull bone.
). The main indication for cranioplasty is the sealing of the tissues of the skull. For this purpose, various transplants (xeno-, allo-, autotransplants) are used. Based on CT and MRI data, it is possible to obtain accurate models that allow modeling an endoprosthesis or implant of the required shape and size in accordance with the missing part of the skull bone. - Training - CT or MRI scans produce high quality and accurate mock-ups to be used as educational and visual aids. Thus, the educational process will be more effective, and the knowledge gained by students can be applied in practice.
If you need to create a model based on MRI or CT image data, to make a physical model, then just contact us. We are sure that we can help you!
How does it work?
You must provide us with the data in digital format. As a rule, this is the DICOM format - a universal format for storing medical graphic data.
Based on the data, using modern surface modeling technology, our employees will quickly create a high-quality 3D model. On average, modeling takes from 1.5 to 3 hours, but the timing is always determined only individually and depends on the initial data, the amount of work and complexity.
On average, modeling takes from 1.5 to 3 hours, but the timing is always determined only individually and depends on the initial data, the amount of work and complexity.
We carry out 3D printing on the equipment we have. In this case, different technologies and materials can be used, selected in accordance with the requirements and tasks to be solved.
Trust our professionalism!
3D printed anatomical models for preoperative planning and enhanced patient consent
Introduction
3D printed models are becoming increasingly useful tools in the modern practice of personalized, precision medicine. As case histories become more complex and treatments become truly unique, visual and tactile anatomical models can improve understanding and communication in the process of creating a solution for a particular patient.
Health care professionals, institutions and organizations around the world use 3D printed anatomical models as reference tools for preoperative planning, intraoperative imaging and calibration or pre-positioning of medical equipment for routine and high complexity procedures, which has been documented in hundreds of publications1. Physicians often save time preparing and performing surgeries, resulting in significant reductions in operating costs while reducing patient risk, anxiety, and recovery time.
Physicians often save time preparing and performing surgeries, resulting in significant reductions in operating costs while reducing patient risk, anxiety, and recovery time.
This guide provides practical step-by-step guidance for physicians and technologists to move from patient scans to 3D printed models by learning how to set up a CT/MRI scan, segment datasets, and convert files to 3D printable format.
“The unique advantage of image-based 3D printing is the ability to demonstrate anatomical spatial relationships with sub-millimeter accuracy.”
Jeffrey D. Hirsch, MD
Associate Professor, Director of Community Radiology, Division of Diagnostic Radiology University of Maryland Medicine
Formlabs-printed anatomy models are already being used by several subspecialists in surgery, including but not limited to orthopedic, cardiothoracic, vascular surgery, oral and maxillofacial surgery, oncology, plastic and reconstructive surgery, urology and pediatrics. This handbook provides an overview of the steps that can be applied to any Digital Imaging and Communications in Medicine (DICOM) dataset, which is the standard format for storing images in any modern Image Archiving and Communication Systems (PACS)
This handbook provides an overview of the steps that can be applied to any Digital Imaging and Communications in Medicine (DICOM) dataset, which is the standard format for storing images in any modern Image Archiving and Communication Systems (PACS)
WHAT YOU NEED FOR IN-HOUSE 3D PRINTING
CT or MRI scan and associated DICOM file
- Recommended slice thickness: 0.25mm-1.25mm2
Computer with imaging software for segmentation or using an outsourced segmentation service
Form 2 3D printer and resin, e.g.:
- Orthopedic white resin or OMFS
- Transparent polymer for cardiovascular or urological surgery
- SG Dental Resin for Surgical Guides (for approved applications only)
Form Wash and Form Cure for 3D post-processing (recommended for medical models)
Applications and benefits of 3D printed anatomical models medicine. Please consider your intended use, local regulations, medical imaging approvals, material specifications, biocompatibility requirements, protected medical information, and institutional standards before 3D printing or using anatomical models
Depending on your institution, anatomical models may be used for patient or pathological purposes:
- Preoperative planning and intraoperative reference models for surgeons
- Device calibration (e.
 g. mandibular plates) and surgical instrument design*
g. mandibular plates) and surgical instrument design* - Molds for implant material or prostheses*
- Teaching and simulation laboratories
- Patient Education and Enhanced Informed Consent
* May be regulated and/or require institutional approval
Numerous published case studies and ongoing efforts have demonstrated the potential of 3D printing in clinical settings. Public use cases include preoperative planning3, intraoperative use4, patient-centric instrument kits5, customized implants6, bone cement molds or polymethyl methacrylate (PMMA) implants8, prostheses9and trays
These use cases have demonstrated success in a variety of fields and surgical specialties, including orthopedic, cardiac, oral and maxillofacial (OMFS), vascular, neurological, cardiothoracic, musculoskeletal, plastic and reconstructive surgery, oncology, pediatrics, interventional radiology, etc.
“While I would like to think that my brain can reconstruct a 3D interpretation from a 2D CT scan, I was surprised by the relative inaccuracy of the approach I have used for 20 years. 3D models are invaluable in planning, especially when using the daVinci robot.”
3D models are invaluable in planning, especially when using the daVinci robot.”
Dr. Ronald Hrebinko
Urologist and Associate Professor of Urology
University of Pittsburgh Department of Medicine
3D printed models can also provide significant benefits for the education of residents, fellows and students10. Individual models are particularly attractive when compared to the cost of cadaveric specimens and animal testing and the associated requirements for laboratory space, surgical instruments, and disposal
5 leading medical disciplines on the use of 3D printing technology
Chepelev et al.
Image sourced from http://www.materialise.com/en/blog/3d-printing-us-hospitals
Explore our collection of research publications, to learn more about how Formlabs printers and supplies are being used in healthcare.
The widespread use of advanced imaging in radiology has become a key factor in diagnosis and communication between physicians. While these visualizations have traditionally been used in the 2D plane as CT or MRI scans as DICOM files, software developers have recently created tools to reconstruct diagnostic images as 3D anatomical imaging.
While these visualizations have traditionally been used in the 2D plane as CT or MRI scans as DICOM files, software developers have recently created tools to reconstruct diagnostic images as 3D anatomical imaging.
3D printed models are a natural extension of these various 3D rendering options and offer many additional benefits such as tactile feedback and other tangible information that visualizations cannot provide.
When a patient's severe foot deformity could not be fully represented with 2D images, surgeons used a 3D printed model to plan how to correct gait with preoperative equipment and work with clinical staff and receptionists.
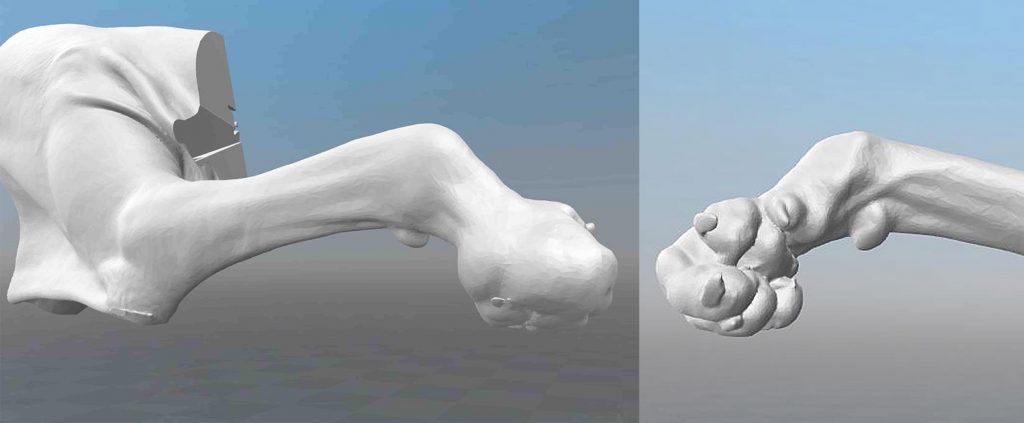
For example, research on a custom 3D printed model allowed a UK orthopedic surgeon to find a solution with a lower risk of abnormal injury to a boy's forearm
“Access to the model has changed standard CT-indicated therapy from a four-hour complex osteotomy to a simple, much less invasive 30-minute soft tissue procedure,” says Dr. Michael Eames
Michael Eames
A successful operation was completed in just 30 minutes — reduction of more than three hours from the originally scheduled time in the operating room, saving the hospital an estimated $5,500. Subsequently, the patient spent less time on post-operative care and recovered more quickly
Scan to 3D model workflows
Creating 3D printed files and 3D printed models requires special considerations and minor changes to the medical imaging workflow
The tailored workflow can be divided into three steps: image acquisition, image segmentation and 3D printing
IMAGE ACQUISITION
Image acquisition is the first step and is already integrated into the workflow. The most common imaging techniques suitable for 3D printing are CT and MRI. In general, 3D models can be printed from any volumetric image dataset (slices) with sufficient contrast to differentiate tissues.
Cone-beam CT is also widely used for dental and otolaryngological imaging of teeth, but contrast can be worse than conventional CT, making segmentation more difficult. See recommendations for setting up patient scans for 3D models in the second part of this booklet
See recommendations for setting up patient scans for 3D models in the second part of this booklet
IMAGE SEGMENTATION
The main goal of this step is to reduce the complexity of the original image while leaving the necessary characteristics unchanged and isolated. Once the radiographer has received the DICOM, they must perform Regions of Interest (ROI) processing, which will be rendered as a 3D printed object. The process of identifying and separating tissues and other areas of interest is called segmentation. Depending on the complexity of the model, it is performed by a radiologist-technician under the guidance of a radiologist or directly by a radiologist. Once the segmentation is completed, it is reviewed by the surgeon for final approval13
A number of commercial and open source software products can be used for the segmentation process (see the list at the end of this section). Before choosing a software solution, consider your intended use, regulatory requirements in your area, and recommendations at your institution.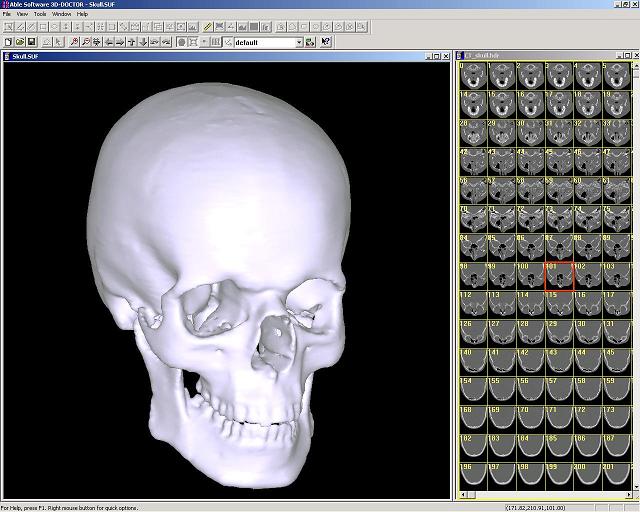
ROI segmentation steps can include automatic methods (eg thresholding, edge detection and region enlargement) or manual selection and adjustments. Thresholding uses parameters that can be identified and associated with a particular ROI, such as bones with higher Hounsfield values relative to their surroundings.
Thresholds may need to be dynamic and include more sophisticated algorithms to account for factors such as CT noise and beam hardening that can create artifacts and other unwanted results.
Another option is to use a growth region to automate segmentation, where the algorithm assigns voxels as belonging to one part or another based on similarity or difference to surrounding voxels. This may require additional adjustments and clarifications.
After segmentation is complete, convert the segmented objects to a file type that can be used by the 3D printer. This file type is usually an STL or OBJ file format.
After conversion, make any necessary physical adjustments that are more common in 3D modeling, such as smoothing surfaces, filling holes, and fixing other minor features. These adjustments can be made by a specialist in various CAD or CAM programs and should always include review by a physician to ensure that the result is clinically useful.
These adjustments can be made by a specialist in various CAD or CAM programs and should always include review by a physician to ensure that the result is clinically useful.
Once the radiographer receives DICOM, they must define regions of interest (ROIs) that will be displayed as a 3D printed object. Source: ITK-Snap
In-house 3D printing allows healthcare providers to quickly create high resolution medical models.
3D PRINT
Once the final file is ready, it can be exported and sent to the 3D printer for production. There are several key factors to consider when choosing the right 3D printing technology, including: the cost of the printer, software, and materials; print speed, accuracy and resolution; ease of use and access to customer service; the type of printed materials, including biocompatibility and sterilization for certain uses.
After printing, parts should be rinsed with isopropyl alcohol (IPA) to remove excess resin and, depending on the material and application, post-cured in a curing chamber. All biocompatible resins require post-cure prior to use, while standard Formlabs resins such as White and Clear Resin increase post-cure strength and stability.
All biocompatible resins require post-cure prior to use, while standard Formlabs resins such as White and Clear Resin increase post-cure strength and stability.
More information about print options
Visit our Software Support and Resources pages for more information on how to set up files for printing and learn more about specifications such as internal supports and minimum wall thickness
POTENTIAL FIELD 3D PRINTING SOFTWARE AND HARDWARE
Note: Each section requires only one kind of software that completes the workflow steps. This list is for ease of reference and research and does not constitute an endorsement of any particular software or vendor. If you require anatomical models without segmentation or printing in situ, specialized service providers offer conversion, segmentation and/or printing services for a fee (e.g. Anatomage, Armor Bionics, Axial3D and Materialize)
Check your local regulations and intended use before choosing a software solution.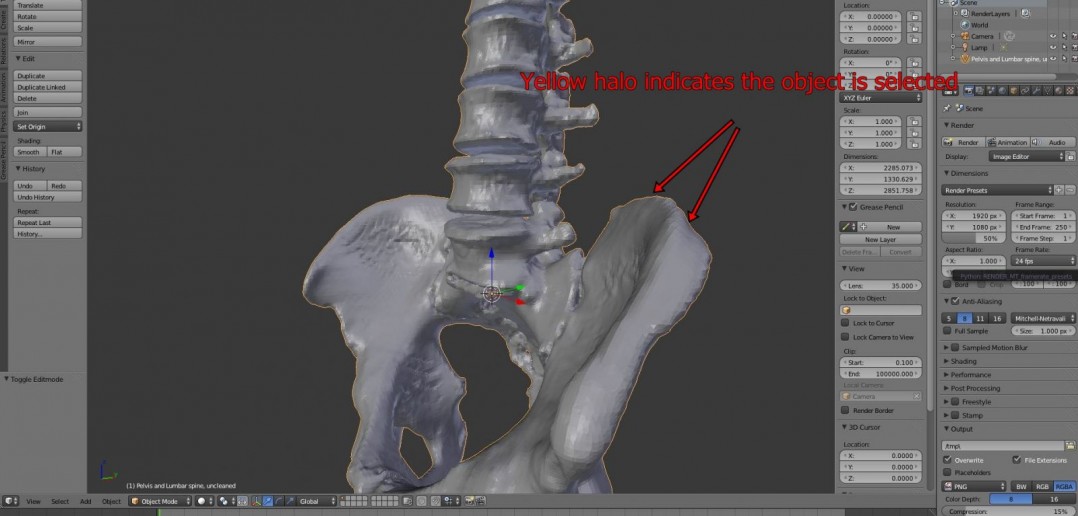
Transform + Segmentation
| Materialise Mimics* | ITK-SNAP |
| 3D Slicer | 4DICOM |
| Axial3D | Seg3D |
| Osirix | Embodi3D (DICOM - STL conversion, no segmentation) |
| Ossa 3D | Vitrea Vital Images |
| Anatomage Medical Design Studio |
Preparation for editing + File management, smoothing and identification
| Blender | Materialize 3matic | Autodesk Meshmixer |
Support Generation + Print Orientation
| Formlabs PreForm | Materialize e-Stage Note: Cardiac cases may require advanced removal of supports from within the valves (PreForm video tutorial) |
Printer
| Formlabs Form 2 or Form Cell system | Formlabs Fuse 1 |
Post-print
| Formlabs finishing kit | Form Wash and Form Cure |
Ultrasonic cleaner (e.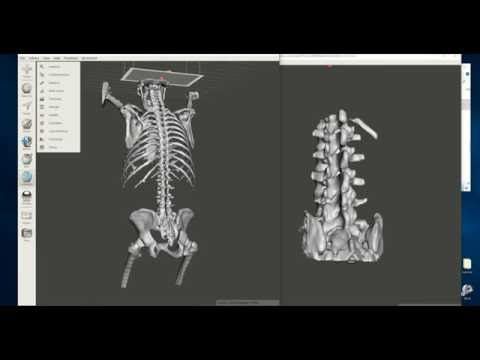 g. GT Sonic) g. GT Sonic) | CUREBox CB-4051 |
* Formlabs and Materialize have partnered to offer a comprehensive package of services in the US, Europe and Japan. Mimics inPrint is a specialized software solution for creating accurate virtual anatomical models from medical images and preparing files for 3D printing. Integrated into Clinical Environments (PACS), Mimics inPrint includes predefined workflows with direct link to Formlabs 3D printers.
Patient Scan Setup for 3D Models
Some conventional medical imaging scans cannot be converted to high quality 3D models for clear and accurate anatomical structures. Plain radiographs (X-rays) and ultrasounds are not commonly used for 3D printing and these imaging techniques are not recommended.
The most commonly used imaging modalities for evaluating internal structures are computed tomography and MRI imaging. These rendering methods generate a DICOM file. DICOM is a standard for storing and transmitting medical images and can be thought of as a series of slices.
DICOM images cannot be edited in 3D design software or sent directly to a printer. To convert a DICOM file to a format suitable for 3D printing, such as an STL or OBJ file, separate software is required to calculate the surface area of interest. This surface will become a 3D model.
Almost any DICOM file with sufficiently fine detail (eg thin slices) can be converted to a format that supports 3D printing of the structure of interest.
The following articles may be helpful in preparing, printing and post-processing anatomy models:
Design models for print support
Design features and geometric recommendations
Post-curing printing
Post-processing basics
Criteria for creating a printable scan
The first consideration when converting a CT or MRI to a 3D model is what needs to be shown; bones, vessels, and whole organs are all modeled differently.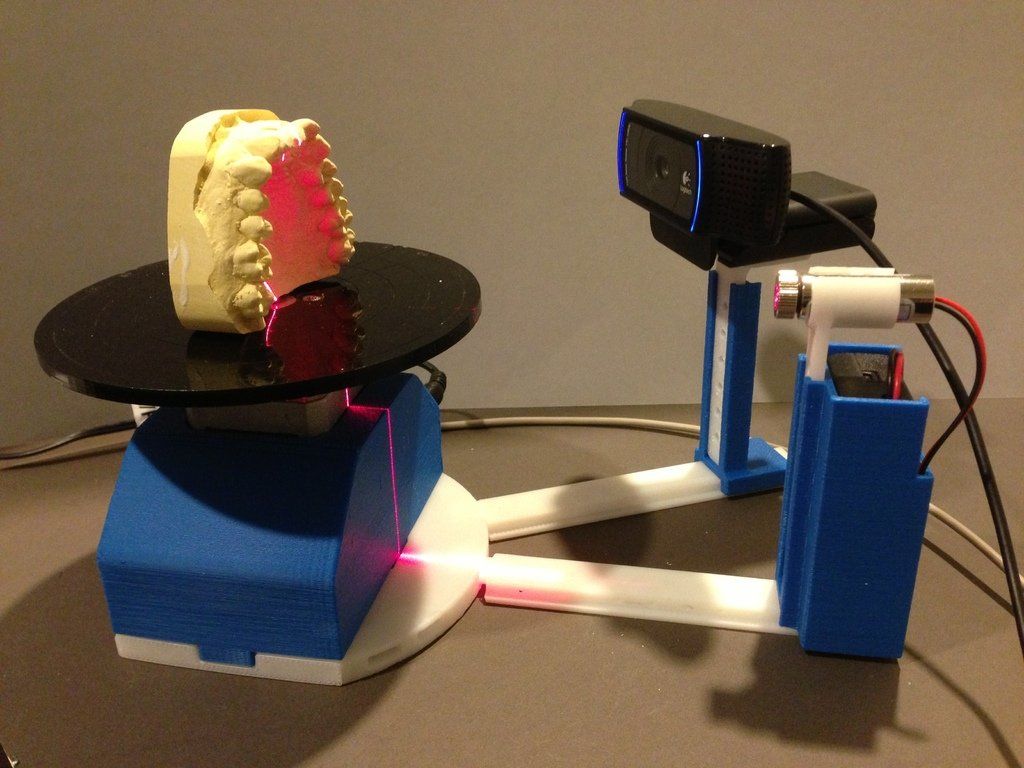 A model with outdated structures not only detracts from the focus of the model, but it will also be harder to produce. Scanning at the right specifications makes it easy to create a 3D printable model. The main features are intravenous contrast and slice thickness.
A model with outdated structures not only detracts from the focus of the model, but it will also be harder to produce. Scanning at the right specifications makes it easy to create a 3D printable model. The main features are intravenous contrast and slice thickness.
For 3D models of bone structures, low contrast images are likely to be sufficient for accurate and detailed printing. Models containing solid organs, tumors, or vascular structures almost always require contrast magnification scans
Introductory contrast information
The CT brightness variation allows the segmentation software to highlight different structures, allowing you to print an area or organ of interest. Some structures, such as bones, are inherently bright on CT scans. This makes it easier to 3D print when started from a non-contrast CT. However, intravenous
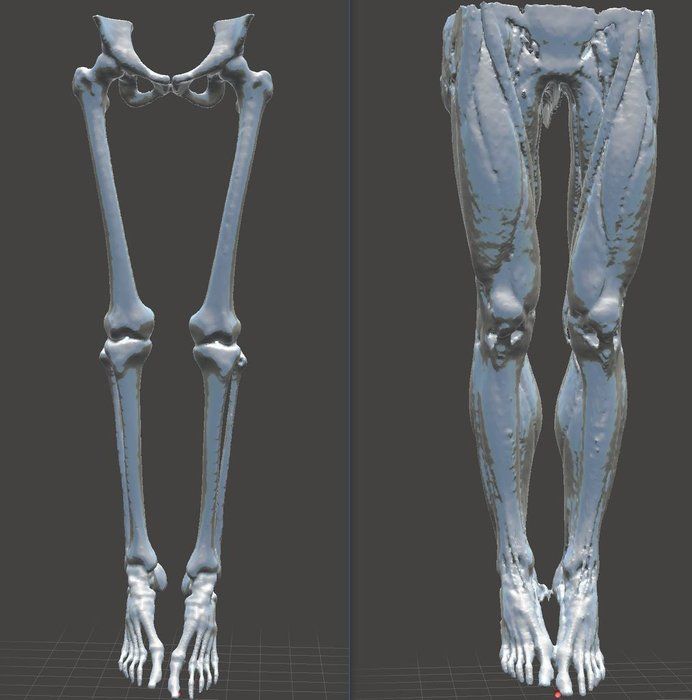
(IV) contrast is needed when you want to 3D print a blood vessel, tumor, or most organs. A contrast agent is injected into the patient just before the scan.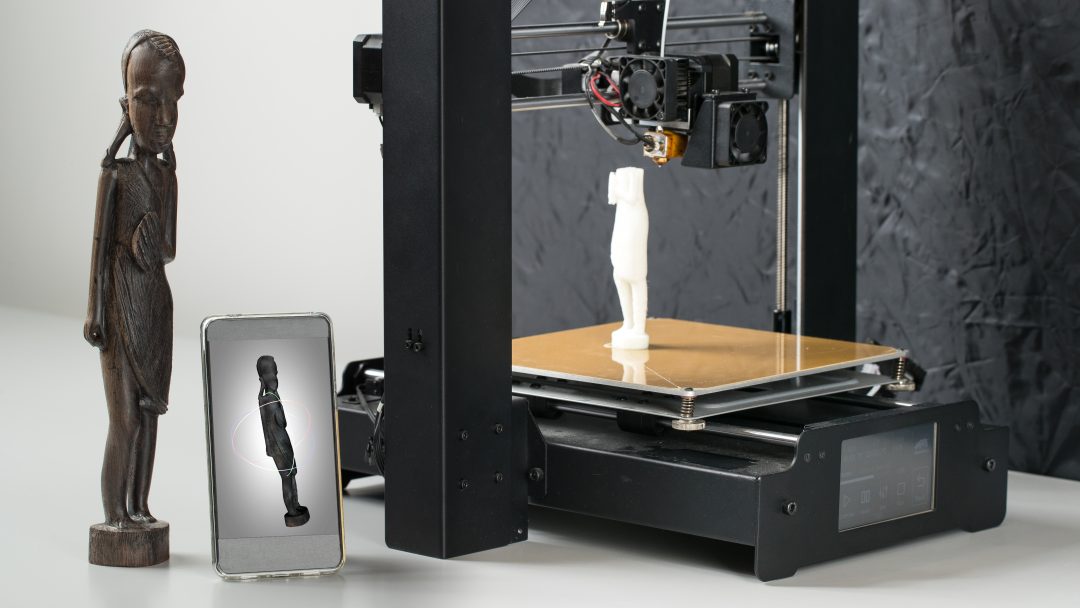 With IV contrast, blood vessels (arteries and veins) and solid organs (such as the liver, kidneys, spleen, heart, and brain) become brighter when scanned, allowing the segmentation software to accurately separate them from surrounding tissues. See images below for a comparison of non-contrast and contrast-enhanced CT scans of the abdomen.
With IV contrast, blood vessels (arteries and veins) and solid organs (such as the liver, kidneys, spleen, heart, and brain) become brighter when scanned, allowing the segmentation software to accurately separate them from surrounding tissues. See images below for a comparison of non-contrast and contrast-enhanced CT scans of the abdomen.
The effect of intravenous contrast is shown with two axial (transverse) CT scans of the upper abdomen. On a right scan, the aorta is enhanced, whereas on a left scan, the aorta appears very similar to the adjacent soft tissue. The contrast allows you to isolate the desired structures in post-processing. Source: Embodi 3D
In addition to enhancing contrast, slice thickness and resolution are equally important for planning when creating a 3D model. Most clinically useful scans were obtained at adequate resolution for 3D printing. However, if you try to 3D print an anatomical model while scanning with thick sections, your
model will have a rough surface. According to numerous sources, when creating a model for 3D printing, it is very important to use scans with slices less than 1.25 mm.
According to numerous sources, when creating a model for 3D printing, it is very important to use scans with slices less than 1.25 mm.
Two CT scans of the chest. The image on the left shows a frontal view constructed from 5 mm thick slices, while the high resolution scan shows a similar view of the chest using only 1 mm thick slices. Thick slices in the left image create rough textures that will result in a lower quality print. Source: Embodi 3D
The thickness of sections obtained from CT or MRI scans are converted directly into details generated from 3D scans. Depending on the focus object, areas of the image should be reconstructed with isotropic voxels of 1.25 mm or less15. According to a Mayo Clinic presentation in March 2016, 1 to 5 mm slices can be used for large structures, while 0.75 mm can be used for thin bone16. Thicker regions may degrade model accuracy, while very thin regions (e.g. <0.25 mm) may require extensive segmentation and STL enhancement, especially in the presence of image artifact. Cardiac models show sufficient accuracy with 0.5 mm patches, but thinner targets may be required for thin objects such as the inferior wall of the orbit17. Generally, thicker areas can create fuzzy or less accurate prints. However, unnecessarily thin areas can lead to significantly more work in the post-processing step.
Cardiac models show sufficient accuracy with 0.5 mm patches, but thinner targets may be required for thin objects such as the inferior wall of the orbit17. Generally, thicker areas can create fuzzy or less accurate prints. However, unnecessarily thin areas can lead to significantly more work in the post-processing step.
Regulatory Issues
Please check local regulations, material data, patient information, and institutional requirements before 3D printing or using anatomical models. If you work in the US, please refer to the latest FDA presentation which outlines its guidance document18 Please note that these documents and recommendations are subject to change. Make sure you are using the latest guidelines.
Formlabs is the industry's leading manufacturer of 3D printers and materials used by healthcare providers to support the practice of medicine
Conclusion
Barriers to the transition to personalized precision medicine are fast disappearing.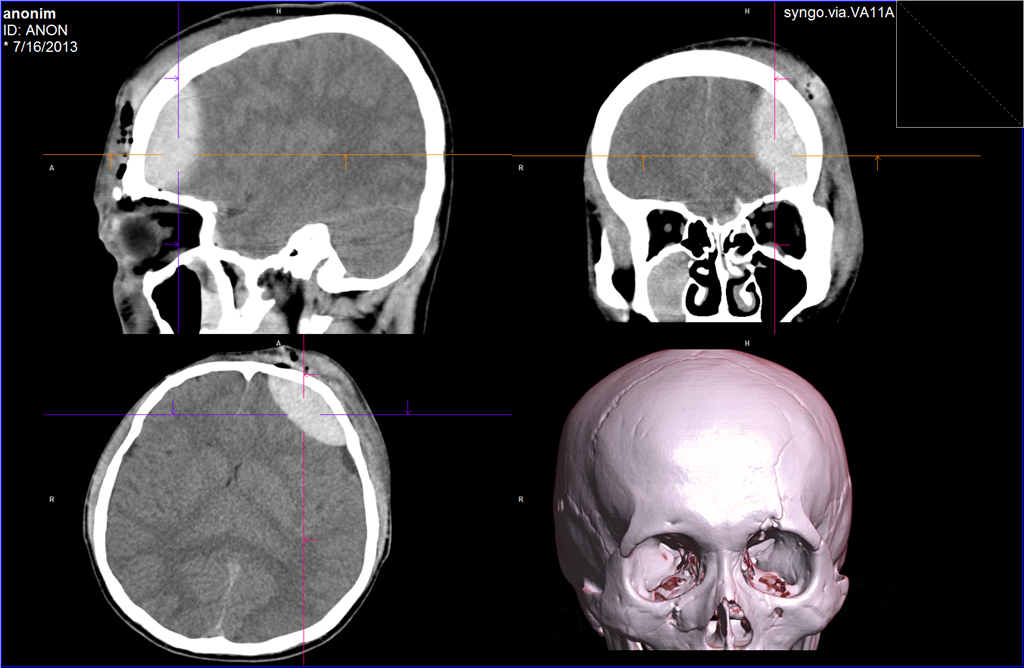 The advent of affordable, professional-grade 3D printers has enabled healthcare providers to produce anatomy models for specific patients and specialties with inspiring results. In some cases, the initial cost of a high quality printer has been covered by the time saved in the operating room after the surgeon used the 3D printed model to prepare for one complex procedure.19
The advent of affordable, professional-grade 3D printers has enabled healthcare providers to produce anatomy models for specific patients and specialties with inspiring results. In some cases, the initial cost of a high quality printer has been covered by the time saved in the operating room after the surgeon used the 3D printed model to prepare for one complex procedure.19
“Medicine is not a one-size-fits-all solution, and when a tool like desktop 3D printing comes along that allows you to create personalized medical solutions, there is no doubt that it needs to be used to its full potential.”
Todd Goldstein
Instructor, Institute for Medical Research. Feinstein Director, 3D Printing Lab, Northwell Ventures, Northwell Health
Understanding the workflow required to integrate 3D printing is key to success.
This tutorial covers everything you need to get started, popular workflows and tools and techniques to ease the transition from patient scanning to 3D printing
Contact us to learn more about 3D printing in Your institution and join the community of innovators in precision medicine
REFERENCES
- Chepelev, Leonid, Andreas Giannopoulos, Anji Tan, Dimitrios Mitsouras, and Frank J.
 Rybicki Medical 3D Printing: Terminology Standardization Techniques and Report Trends 3D- printing in medicine 3, no. 1 (2017) doi:101186/s41205-017-0012-5
Rybicki Medical 3D Printing: Terminology Standardization Techniques and Report Trends 3D- printing in medicine 3, no. 1 (2017) doi:101186/s41205-017-0012-5 - Mitsworth, Dimitris, Peter Lakouras, Amir Imanzadeh, Andreas A Giannopoulos, Tianrun Kai, Kanako K. Kumamaru, Elizabeth George, et al. "3D Medical Printing for the Radiologist" RadioGraphics 35, no. 7 (November 2015): 1965–88 https ://doi.org/101148/rg2015140320
- Kerr, William, Philip Rowe, and Steven Gareth Pierce "Accurate 3D Bone Reconstruction Using Ultrasonic Synthetic Aperture Techniques for Robotic Knee Arthroplasty" Computerized Medical Imaging and Graphics 58 (June 2017): 23–32 https://doi org/101016/j compmedimag 201703 002
- Chen, Xing, Jesse K Possel, Katherine Waconne, Ann F van Ham, P. Christian Klink, and Peter R. Roelfsema "3D printing and modeling of customized implants and surgical guides for lower primates" Journal of Neuroscience Methods 286 (July 2017 ): 38–55 https://doi org/101016/jjneumeth 201705 013
- Wong, K.
 S., S.M. Kumta, N. V. Geel and J. Demol "One-stage reconstruction with a 3D printed, biomechanically assessed custom implant after complex resection of pelvic tumors" Computer Surgery 20, no. 1 (January 2, 2015): 14–23 https:// doi org/10 3109/1092908820151076039
S., S.M. Kumta, N. V. Geel and J. Demol "One-stage reconstruction with a 3D printed, biomechanically assessed custom implant after complex resection of pelvic tumors" Computer Surgery 20, no. 1 (January 2, 2015): 14–23 https:// doi org/10 3109/1092908820151076039 - Tan, Eddy T.V., Ji Ming Lin, and Shri Kumar Dinesh “Creating Acrylic Patient Cranioplasty Implants with an Inexpensive 3D Printer” Journal of Neurosurgery 124, no. 5 (May 2016): 1531–37 https://doi org/10 3171/2015 5 jns15119
- Tan, Eddy T.V., Ji Ming Lin, and Shri Kumar Dinesh “Creating Acrylic Patient Cranioplasty Implants with an Inexpensive 3D Printer” Journal of Neurosurgery 124, no. 5 (May 2016): 1531–37 https://doi org/10 3171/2015 5 jns15119
- Abdel Hey, Joe, Tarek Smyra, and Ronald Moussa "Customized Implants with PMMA Cranioplasty Using 3D Polylactic Acid Printing Plates: Technical Note with 2 Illustrative Examples" World Neurosurgery 105 (September 2017): 971–979 e1 https http://doi.org/101016/j wneu 201705 00
- Keith, Jelleten, Gerwyn Smith, and Paul Bredveld, 3D Printed Upper Limb Prosthesis: An Overview of Disability and Rehabilitation: Rehabilitation Techniques 12, no.
 3 (February 2, 2017): 300–314 https://doi org/ 101080/1748310720161253117
3 (February 2, 2017): 300–314 https://doi org/ 101080/1748310720161253117 - Azer, Sami A., and Sara Azer, “3D Anatomical Models and Impact on Learning: A Review of Quality in the Literature,” Health Professions Education 2, no. 2 (December 2016): 80–98 https://doi org/101016 /j hpe 2016 05 002
- Planning with a Custom Surgical Model Reduces OR Time by 88 Percent Formlabs Accessed November 22, 2017 https://formlabs com/preoperative-planning-with-custom-3d-printed-surgical-model-reduces-theater-time/
- Christensen, Andy "Medical Imaging Software" 3D printing | Wohlers Associates Accessed November 22, 2017 http://www.wohlersassociates com/
- Matsumoto, Jane S., Jonathan M. Morris, Thomas Foley, Eric E. Williamson, Shuai Leng, Ciarán P McGay, Joel L. Kuhlmann, Linda E. Nesberg, and Terry J. Vrtiska 3D Physical Modeling: Applications and Experiences in Mayo Clinic RadioGraphics 35, No. 7 (2015): 1989-2006 doi:101148/rg 2015140260
- Kikinis R, Piper SD, Vosburg K.
 (2014) 3D Slicer: a platform for subject image analysis, visualization and clinical support. Intraoperative image processing. Imaging Therapy, Ferenc A. Jolez, Editor 3 (19): 277-289 ISBN : 978-1-4614-7656-6 (Print) 978-1-4614-7657-3 (Online) https://www slicerorg/wiki/ CitingSlicer
(2014) 3D Slicer: a platform for subject image analysis, visualization and clinical support. Intraoperative image processing. Imaging Therapy, Ferenc A. Jolez, Editor 3 (19): 277-289 ISBN : 978-1-4614-7656-6 (Print) 978-1-4614-7657-3 (Online) https://www slicerorg/wiki/ CitingSlicer - Mitsworth, Dimitris, Peter Lakouras, Amir Imanzadeh, Andreas A Giannopoulos, Tianrun Kai, Kanako K. Kumamaru, Elizabeth George, et al. "3D Medical Printing for the Radiologist" RadioGraphics 35, no. 7 (November 2015): 1965–88 https ://doi.org/101148/rg2015140320
- TJ Vrtiska, MD, Jane Matsumoto, MD, Jay Morris, MD, Imaging: The Role of the Radiologist. A Key First Step” Mayo Clinic (March 4, 2016)
- Mitsworth, Dimitris, Peter Lakouras, Amir Imanzadeh, Andreas A Giannopoulos, Tianrun Kai, Kanako K. Kumamaru, Elizabeth George, et al. "3D Medical Printing for the Radiologist" RadioGraphics 35, no. 7 (November 2015): 1965–88 https ://doi.org/101148/rg2015140320
- Nooshin Kiarashi, PhD, FDA/CDRH/Department of Radiological Medicine, "FDA Current Practice and Regulations, FDA/CDRH-RSNA SIG Joint Meeting on Customized 3D Printed Anatomical Models", excerpted from https://www fda gov/ downloads/MedicalDevices/NewsEvents/WorkshopsConferences/ UCM575723 pdf
- Preoperative-planning-with-custom-3d-printed-surgical-model-reduces-theater-time by 88 percent Formlabs Accessed November 22, 2017
ADDITIONAL RESOURCES AND LINKS
1531–37 https://doi org/10 3171/2015 5 jns15119 Kikinis R. , Pieper S. D., Vosburg K. (2014) 3D Slicer: A Platform for Objective Image Analysis , imaging and clinical support. Intraoperative image processing. Imaging Therapy, Ferenc A. Jolez, Editor 3 (19): 277-289 ISBN : 978-1-4614-7656-6 (Print) 978-1-4614-7657-3 (Online)
, Pieper S. D., Vosburg K. (2014) 3D Slicer: A Platform for Objective Image Analysis , imaging and clinical support. Intraoperative image processing. Imaging Therapy, Ferenc A. Jolez, Editor 3 (19): 277-289 ISBN : 978-1-4614-7656-6 (Print) 978-1-4614-7657-3 (Online)
Rybicki F. Christensen, A. (05/12/2017) Recommendations for Medical 3D print: Patient safety. Retrieved Nov 03, 2017 from https://www 3printrcom/ guidelines-medical-3d-printing-patient- safety-3345869/ (n d ) http://www conceptualiz com/resources html
Biomedical Modeling, Inc Materials (16.10 .2013) Biomodeling process: From 2D to 3D https://www slideshare net/Biomedical_Modeling_Inc/the- biomodeling-process-from-2d-to-3d-27259255
Choosing the Best Medical Imaging Scan for a 3D Printed Medical Model (December 27, 2016) https://www embodi3d com/blogs/entry/183-choosing-the-best-medical-imaging-scan-to- create-a-3d-printed-medical-model/
Documentation/4 6/Training (n d ) https://www slicerorg/wiki/ Documentation/4.