Cost of 3d printed knee replacement
Medical 3D Printing Cost-savings in Orthopedic and Maxillofacial Surgery: Cost Analysis of Operating Room Time Saved with 3D Printed Anatomic Models and Surgical Guides
1. New ACR-Sponsored CPT Codes Approved by the AMA. American College of Radiology Website. Available at: https://www.acr.org/Advocacy-and-Economics/Advocacy-News/Advocacy-News-Issues/In-the-November-2-2018-Issue/New-ACR-Sponsored-CPT-Codes-Approved-by-the-AMA Accessed August 20, 2019.
2. Most recent changes to the CPT®) Category III Codes document. American Medical Association Website. Available at: https://www.ama-assn.org/system/files/2019-03/cpt-category3-codes-long-descriptors.pdf Accessed August 20, 2019.
3. Hirsch JA, Leslie-Mazwi TM, Nicola GN, et al. Current procedural terminology; a primer. J Neurointerv Surg 2015;7:309–312. [PubMed] [Google Scholar]
4. RSNA and ACR to Collaborate on Landmark Medical 3D Printing Registry. Radiological Society of North America Website. Available at: https://www. rsna.org/en/news/2019/August/3D-Printing-Registry Accessed August 20, 2019.
5. Chepelev L, Wake N, Ryan J, et al. Radiological Society of North America (RSNA) 3D printing Special Interest Group (SIG): guidelines for medical 3D printing and appropriateness for clinical scenarios. 3D Print Med 2018; 4:11. [PMC free article] [PubMed] [Google Scholar]
6. Ballard DH, Trace AP, Ali S, et al. Clinical Applications of 3D Printing: Primer for Radiologists. Acad Radiol 2018;25:52–65. [PMC free article] [PubMed] [Google Scholar]
7. Hodgdon T, Danrad R, Patel MJ, et al. Logistics of Three-dimensional Printing: Primer for Radiologists. Acad Radiol 2018;25:40–51. [PMC free article] [PubMed] [Google Scholar]
8. D’Urso PS, Barker TM, Earwaker WJ, et al. Stereolithographic biomodelling in craniomaxillofacial surgery: a prospective trial. J Craniomaxillofac Surg 1999;27:30–37. [PubMed] [Google Scholar]
9. Tack P, Victor J, Gemmel P, Armenians L. 3D-printing techniques in a medical setting: a systematic literature review. Biomed Eng Online 2016; 15:115. [PMC free article] [PubMed] [Google Scholar]
Biomed Eng Online 2016; 15:115. [PMC free article] [PubMed] [Google Scholar]
10. Martelli N, Serrano C, van den Brink H, et al. Advantages and disadvantages of 3-dimensional printing in surgery: A systematic review. Surgery 2016; 159:1485–1500. [PubMed] [Google Scholar]
11. George E, Liacouras P, Rybicki FJ, Mitsouras D. Measuring and Establishing the Accuracy and Reproducibility of 3D Printed Medical Models. Radiographics 2017;37:1424–1450. [PMC free article] [PubMed] [Google Scholar]
12. Crump SS. Apparatus and method for creating three-dimensional objects. US Patent 5,121,329; October 30, 1989. [Google Scholar]
13. Rybicki FJ. Medical 3D printing and the physician-artist. Lancet 2018;391:651–652. [PubMed] [Google Scholar]
14. Collins FS, Varmus H. A new initiative on precision medicine. N Engl J Med 2015;372:793–795. [PMC free article] [PubMed] [Google Scholar]
15. Shippert RD. A Study of Time-Dependent Operating Room Fees and How to save $100 000 by Using Time-Saving Products.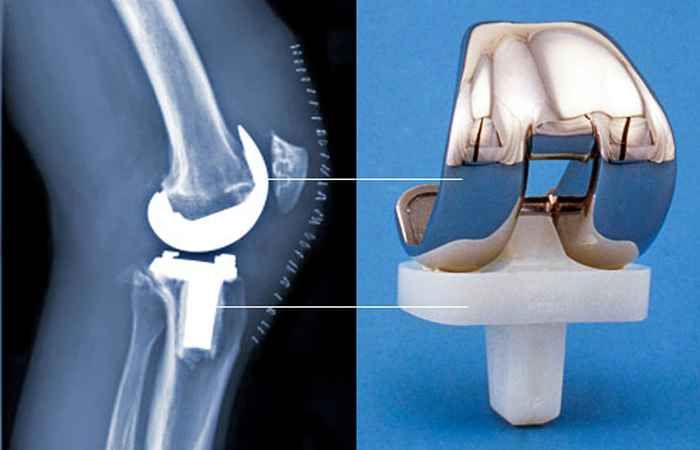 The American Journal of Cosmetic Surgery 2005;22:25–34. [Google Scholar]
The American Journal of Cosmetic Surgery 2005;22:25–34. [Google Scholar]
16. Resnick AS, Corrigan D, Mullen JL, Kaiser LR. Surgeon contribution to hospital bottom line: not all are created equal. Ann Surg 2005;242:530–537; discussion 537-539. [PMC free article] [PubMed] [Google Scholar]
17. Sieira Gil R, Roig AM, Obispo CA, Morla A, Pages CM, Perez JL. Surgical planning and microvascular reconstruction of the mandible with a fibular flap using computer-aided design, rapid prototype modelling, and precontoured titanium reconstruction plates: a prospective study. Br J Oral Maxillofac Surg 2015;53:49–53. [PubMed] [Google Scholar]
18. Xu H, Zhang C, Shim YH, Li H, Cao D. Combined use of rapid-prototyping model and surgical guide in correction of mandibular asymmetry malformation patients with normal occlusal relationship. J Craniofac Surg 2015:26:418–421. [PubMed] [Google Scholar]
19. de Farias TP, Dias FL, Galvão MS, Boasquevisque E, Pastl AC, Albuquerque Sousa B. Use of prototyping in preoperative planning for patients with head and neck tumors. Head Neck 2014;36:1773–1782. [PubMed] [Google Scholar]
Head Neck 2014;36:1773–1782. [PubMed] [Google Scholar]
20. Hanasono MM, Skoracki RJ. Computer-assisted design and rapid prototype modeling in microvascular mandible reconstruction. Laryngoscope 2013;123:597–604. [PubMed] [Google Scholar]
21. Zhang S, Liu X, Xu Y, et al. Application of rapid prototyping for temporomandibular joint reconstruction. J Oral Maxillofac Surg 2011;69:432–438. [PubMed] [Google Scholar]
22. Zhang YZ, Chen B, Lu S, et al. Preliminary application of computer-assisted patient-specific acetabular navigational template for total hip arthroplasty in adult single development dysplasia of the hip. Int J Med Robot 2011;7:469–474. [PubMed] [Google Scholar]
23. Yang M, Li C, Li Y, et al. Application of 3D rapid prototyping technology in posterior corrective surgery for Lenke 1 adolescent idiopathic scoliosis patients. Medicine (Baltimore) 2015;94:e582. [PMC free article] [PubMed] [Google Scholar]
24. Toto JM, Chang El, Agag R, Devarajan K, Patel SA, Topham NS. Improved operative efficiency of free fibula flap mandible reconstruction with patient-specific, computer-guided preoperative planning. Head Neck 2015;37:1660–1664. [PubMed] [Google Scholar]
Improved operative efficiency of free fibula flap mandible reconstruction with patient-specific, computer-guided preoperative planning. Head Neck 2015;37:1660–1664. [PubMed] [Google Scholar]
25. Hsu AR, Davis WH, Cohen BE, Jones CP, Ellington JK, Anderson RB. Radiographic Outcomes of Preoperative CT Scan-Derived Patient-Specific Total Ankle Arthroplasty. Foot Ankle Int 2015;36:1163–1169. [PubMed] [Google Scholar]
26. Chareancholvanich K, Narkbunnam R, Pomrattanamaneewong C. A prospective randomised controlled study of patient-specific cutting guides compared with conventional instrumentation in total knee replacement. Bone Joint J 2013;95-B:354–359. [PubMed] [Google Scholar]
27. Abane L, Anract P, Boisgard S, Descamps S, Courpied JP, Hamadouche M. A comparison of patient-specific and conventional instrumentation for total knee arthroplasty: a multicentre randomised controlled trial. Bone Joint J 2015;97-B:56–63. [PubMed] [Google Scholar]
28. Barrack RL, Ruh EL, Williams BM, Ford AD, Foreman K, Nunley RM. Patient specific cutting blocks are currently of no proven value. J Bone Joint Surg Br 2012;94:95–99. [PubMed] [Google Scholar]
Patient specific cutting blocks are currently of no proven value. J Bone Joint Surg Br 2012;94:95–99. [PubMed] [Google Scholar]
29. Barrett W, Hoeffel D, Dalury D, Mason JB, Murphy J, Himden S. In-vivo alignment comparing patient specific instrumentation with both conventional and computer assisted surgery (CAS) instrumentation in total knee arthroplasty. J Arthroplasty 2014;29:343–347. [PubMed] [Google Scholar]
30. Boonen B, Schotanus MGM, Kort NP. Preliminary experience with the patient-specific templating total knee arthroplasty. Acta Orthop 2012;83:387–393. [PMC free article] [PubMed] [Google Scholar]
31. Boonen B, Schotanus MGM, Kerens B, van der Weegen W, van Drumpt R a M, Kort NP. Intraoperative results and radiological outcome of conventional and patient-specific surgery in total knee arthroplasty: a multicentre, randomised controlled trial. Knee Surg Sports Traumatol Arthrosc 2013;21:2206–2212. [PubMed] [Google Scholar]
32. Ferrara F, Cipriani A, Magarelli N, et al. Implant positioning in TKA: comparison between conventional and patient-specific instrumentation. Orthopedics 2015;38:e271–280. [PubMed] [Google Scholar]
Implant positioning in TKA: comparison between conventional and patient-specific instrumentation. Orthopedics 2015;38:e271–280. [PubMed] [Google Scholar]
33. Gan Y, Ding J, Xu Y, Hou C. Accuracy and efficacy of osteotomy in total knee arthroplasty with patient-specific navigational template. Int J Clin Exp Med 2015;8:12192–12201. [PMC free article] [PubMed] [Google Scholar]
34. Hamilton WG, Parks NL, Saxena A. Patient-specific instrumentation does not shorten surgical time: a prospective, randomized trial. J Arthroplasty 2013;28:96–100. [PubMed] [Google Scholar]
35. Kassab S, Pietrzak WS. Patient-specific positioning guides versus manual instrumentation for total knee arthroplasty: an intraoperative comparison. J Surg Orthop Adv 2014;23:140–146. [PubMed] [Google Scholar]
36. Kerens B, Schotanus MGM, Boonen B, Kort NP. No radiographic difference between patient-specific guiding and conventional Oxford UKA surgery. Knee Surg Sports Traumatol Arthrosc 2015;23:1324–1329.![]() [PubMed] [Google Scholar]
[PubMed] [Google Scholar]
37. Nankivell M, West G, Pourgiezis N. Operative efficiency and accuracy of patient-specific cutting guides in total knee replacement. ANZ J Surg 2015:85:452–455. [PubMed] [Google Scholar]
38. Noble JW, Moore CA, Liu N. The value of patient-matched instrumentation in total knee arthroplasty. J Arthroplasty 2012;27:153–155. [PubMed] [Google Scholar]
39. Nunley RM, Ellison BS, Ruh EL, et al. Are patient-specific cutting blocks cost-effective for total knee arthroplasty? Clin Orthop Relat Res 2012;470:889–894. [PMC free article] [PubMed] [Google Scholar]
40. Pfitzner T, Abdel MP, von Roth P, Perka C, Hommel H. Small improvements in mechanical axis alignment achieved with MRI versus CT-based patient-specific instruments in TKA: a randomized clinical trial. Clin Orthop Relat Res 2014;472:2913–2922. [PMC free article] [PubMed] [Google Scholar]
41. Pietsch M, Djahani O, Zweiger C, et al. Custom-fit minimally invasive total knee arthroplasty: effect on blood loss and early clinical outcomes. Knee Surg Sports Traumatol Arthrosc 2013;21:2234–2240. [PubMed] [Google Scholar]
Knee Surg Sports Traumatol Arthrosc 2013;21:2234–2240. [PubMed] [Google Scholar]
42. Rathod PA, Deshmukh AJ, Cushner FD. Reducing blood loss in bilateral total knee arthroplasty with patient-specific instrumentation. Orthop Clin North Am 2015;46:343–350, ix. [PubMed] [Google Scholar]
43. Renson L, Poilvache P, Van den Wyngaert H. Improved alignment and operating room efficiency with patient-specific instrumentation for TKA. Knee 2014;21:1216–1220. [PubMed] [Google Scholar]
44. Roh YW, Kim TW, Lee S, Seong SC, Lee MC. Is TKA using patient-specific instruments comparable to conventional TKA? A randomized controlled study of one system. Clin Orthop Relat Res 2013;471:3988–3895. [PMC free article] [PubMed] [Google Scholar]
45. Lethaus B, Poort L, Bockmann R, Smeets R, Tolba R, Kessler P. Additive manufacturing for microvascular reconstruction of the mandible in 20 patients. J Craniomaxillofac Surg 2012;40:43–46. [PubMed] [Google Scholar]
46. Weinstock P, Prabhu SP, Flynn K, Orbach DB, Smith E. Optimizing cerebrovascular surgical and endovascular procedures in children via personalized 3D printing. J Neurosurg Pediatr 2015;16:584–589. [PubMed] [Google Scholar]
Optimizing cerebrovascular surgical and endovascular procedures in children via personalized 3D printing. J Neurosurg Pediatr 2015;16:584–589. [PubMed] [Google Scholar]
47. Izatt MT, Thorpe PLPJ, Thompson RG, et al. The use of physical biomodelling in complex spinal surgery. Eur Spine J 2007;16:1507–1518. [PMC free article] [PubMed] [Google Scholar]
48. Kunz M, Rudan JF, Xenoyannis GL, Ellis RE. Computer-assisted hip resurfacing using individualized drill templates. J Arthroplasty 2010;25:600–606. [PubMed] [Google Scholar]
49. Hananouchi T, Saito M, Koyama T, et al. Tailor-made surgical guide based on rapid prototyping technique for cup insertion in total hip arthroplasty. Int J Med Robot 2009;5:164–169. [PubMed] [Google Scholar]
50. Zinser M, Zoeller J. Computer-Designed Splints for Surgical Transfer of 3D Orthognathic Planning. Facial Plast Surg 2015;31:474–490. [PubMed] [Google Scholar]
51. Mihalko WM. Patient-Specific Cutting Guides Were Not Better Than Conventional Instrumentation for Total Knee Arthroplasty. J Bone Joint Surg Am 2015;97:1891. [PubMed] [Google Scholar]
J Bone Joint Surg Am 2015;97:1891. [PubMed] [Google Scholar]
52. Goggans TP. Break-even analysis with curvilinear functions. The Accounting Review 1965;40:867–871. [Google Scholar]
53. Diment LE, Thompson MS, Bergmann JHM. Clinical efficacy and effectiveness of 3D printing: a systematic review. BMJ Open 2017;7:e016891. [PMC free article] [PubMed] [Google Scholar]
54. Witowski J, Sitkowski M, Zuzak T, et al. From ideas to long-term studies: 3D printing clinical trials review. Int J Comput Assist Radiol Surg 2018;13:1473–1478. [PMC free article] [PubMed] [Google Scholar]
55. Torres 10, De Luccia N. A simulator for training in endovascular aneurysm repair: The use of three dimensional printers. Eur J Vase Endovasc Surg 2017;54:247–253. [PubMed] [Google Scholar]
56. Obasare E, Mainigi SK, Morris DL, et al. CT based 3D printing is superior to transesophageal echocardiography for pre-procedure planning in left atrial appendage device closure. Int J Cardiovasc Imaging 2018;34:821–831. [PubMed] [Google Scholar]
[PubMed] [Google Scholar]
57. Ryan J, Plasencia J, Richardson R, et al. 3D printing for congenital heart disease: a single site’s initial three-year experience. 3D Print Med 2018;4:10. [PMC free article] [PubMed] [Google Scholar]
58. Childers CP, Maggard-Gibbons M. Understanding Costs of Care in the Operating Room. JAMA Surg 2018;153:el76233. [PMC free article] [PubMed] [Google Scholar]
59. Consumer Price Index Inflation Calculator. U.S. Bureau of Labor Statistics; Available at: https://data.bls.gov/cgi-bin/cpicalc.pl Accessed: August 20, 2019. [Google Scholar]
How 3D printing and robots improve knee replacement surgery
Stryker’s Triathlon implant has four components (from top): femur, patella (attached to the femur), liner, and tibia. Images: Stryker
Total knee replacement surgery has intrigued me since 1979, when my grandfather had the procedure performed on both knees. The prostheses of that era were designed to anatomically mimic the motion of a knee joint, making them superior to their hinge-action predecessors of the ’60s.
But as I’ve discovered since undergoing my own knee replacement surgery last November, today’s prostheses, surgical techniques, and patient outcomes have vastly improved since Gramps was rolled into the operating room. Advancements in what’s medically known as total knee arthroplasty (TKA) include materials developed specifically for implants and their 3D-printed components, as well as the use of surgical-assist robots.
To learn more about TKA and 3D printing’s role in producing implants, I contacted Stryker Corp., the manufacturer of my new knee and the robot that assisted with its implantation.
I spoke with Robert Cohen, president of Stryker’s Digital, Robotics, and Enabling Technologies entity. Cohen, who earned multiple engineering degrees at New Jersey Institute of Technology in the 1980s, has spent his career manufacturing implants. He also has unfettered enthusiasm for how digital technologies like 3D printing help engineers improve TKA surgery, with “help” being the operative word.
He describes additive manufacturing as a “tool” that aids engineers in discovering solutions to problems that can’t be solved by conventional manufacturing methods. “3D printing by itself is nothing but fancy printing—another way to manufacture.”
What drives innovation are the “skillsets of people who want to solve problems in new ways and come up with, in our case, new implants. 3D printing is the enabler that [makes their] designs reality,” he said.
Stryker began adopting additive manufacturing technologies in 2002. Besides knees, the global corporation headquartered in Kalamazoo, Mich., also 3D-prints hips, spinal cages, and other implantable devices. AM allows the company to produce prosthetic geometries that would be impossible or impractical to manufacture by traditional methods. An example is additively manufactured scaffolds that promote biologic fixation—the growth of bone into a prosthetic.
“3D printing is the only way to do that,” said Cohen. “Bone wants to grow into something. Instead of just doing a line-of-sight process, where you might drill holes, and say, ‘Hey, bone, I hope you grow into the holes.’ Now we can print a scaffold structure and bone will grow into it, and the scaffold has structural integrity at the same time. Just like a railroad trestle.”
Instead of just doing a line-of-sight process, where you might drill holes, and say, ‘Hey, bone, I hope you grow into the holes.’ Now we can print a scaffold structure and bone will grow into it, and the scaffold has structural integrity at the same time. Just like a railroad trestle.”
Growth of TKAs
I wasn’t the only passenger who boarded the TKA train last year. It’s estimated that more than 600,000 Americans annually receive the surgery—a figure expected to rise in the coming decade. The combined number of hip and knee replacement procedures in the U.S. is about 1 million yearly.
My surgical team at NorthShore Medical Group-Skokie, outside Chicago, used Stryker’s Triathlon total knee system and was assisted by the medical device manufacturer’s Mako surgical robot. The cementless implant incorporates a femur, tibia, patella, and polyethylene liner.
The Triathlon’s additive components are made from a titanium alloy Stryker developed for 3D printing.
The use of cementless knees has grown rapidly the past few years. The reason is because bone cement, long used for TKA surgeries, is an interface that can break down, said Cohen. “It’s another opportunity for the implant to loosen.”
Stryker casts the femoral component of a Triathlon knee from cobalt chromium, a material that interacts well with the plastic liner. After casting, the femur is finish-machined and coated with sintering beads that promote bone ingrowth.
During TKA surgery, a series of box cuts are made on the patient’s femur. The two cuts on the end interface with the implant like a wedge being pounded into a piece of wood. “That’s the most stable surface ever,” said Cohen. “Think about it. You’re standing up, so you’re always sort of pushing the [bone] tighter into place.”
Producing the patella is a comparatively straightforward process. The metal-backed patella is fitted with a 3D-printed geometry made from Tritanium, a titanium alloy Stryker developed specifically for AM applications in which bone ingrowth is desirable.
Tritanium also is used to 3D-print the tibial baseplate. It forms a virtually fail-proof bond with the patient’s tibia using an interference-fit connection, a force that relies on friction to hold together two mating, tightly fitting objects. The main features of the metal baseplate’s design are four pegs and a keel.
Cohen said, “With additive manufacturing, we can put those posts and keel where they’ll all work together to create an interference fit.” It is “rock solid.” He added that machining the baseplate couldn’t be justified economically. “The cost would be outlandish.”
Manufacturing Overview
For AM applications, Stryker mostly uses direct metal laser sintering (DMLS) printers. “We were doing some electron-beam processes for larger metal parts,” said Cohen, “and we’re looking at different printers for [complex] jigs and fixtures and for disposable instruments and polymers. There are some polymers that could be used for an implant, and there are some polymers that could be single-use surgical instruments, depending on the material requirements. ”
”
Selecting and bringing a 3D printer online to build prostheses is a major undertaking. In the world of metal load-bearing implants, it would be unrealistic to buy a DMLS printer, plug it in, and expect to make an implant.
Printing metal implants requires learning to control the laser, melt pool, wattage and feeds, layering, and many other process parameters. “Because we’ve built competencies in those areas,” said Cohen, “we’re one of the few companies in health care, in the world, that has the capability to scale up and not just do small-run production.”
The corporation’s scaling capabilities have been augmented by its AMagine Institute, a global technology development center located in Cork, Ireland. Reportedly the world’s largest facility dedicated to additively manufacturing orthopedic components, Cohen said the institute’s production personnel 3D-print more than 1 million parts annually.
A view of how implant components fit on a patient.
Robot-Assisted Surgeries
A much smaller though equally impressive sum is 1,000—the number of Mako robot-assist systems Stryker has placed in hospitals the past three years. A Mako robot, which costs more than $1 million, according to published reports, is used to implant Triathlon knees. The system determines final bone preparation and implantation steps to be executed with special Triathlon instruments.
Cohen said 42% of the primary knees that Stryker sells in the United States are implanted with a Mako robot. He expects the percentage to rise to 50% soon.
As is the case with learning to 3D-print TKA components, developing a surgical robot isn’t a task for the impatient or inexperienced. Cohen said, “We design the robots. We write the software, and we build the robots ourselves because nobody else can do it. We have worked on this for over a decade.”
A key benefit of the robotic system is that it provides the surgical team unprecedented amounts of data about the patient’s knee before and during surgery. The process starts with the hospital taking a CT scan of a patient’s knee prior to admittance. The hospital sends the scan to Stryker, which creates a virtual 3D model of the knee joint, tibia, femur, patella, cartilage, and ligaments. The scan also reveals useful information like the amount of arthritic damage the patient has incurred and joint-space narrowing caused by cartilage loss.
The process starts with the hospital taking a CT scan of a patient’s knee prior to admittance. The hospital sends the scan to Stryker, which creates a virtual 3D model of the knee joint, tibia, femur, patella, cartilage, and ligaments. The scan also reveals useful information like the amount of arthritic damage the patient has incurred and joint-space narrowing caused by cartilage loss.
The next step is to match the data with a virtual implant. Stryker team members position virtual models of the femur and tibia on the virtual bones and gather data on rotation, X-Y-Z axes, tilt, slant—“everything you could possibly need to match you is individualized,” Cohen explained. The team also re-establishes the patient’s joint line, in three dimensions.
“The purpose of the robot is to get your knee exactly on your joint line … and to make surfaces that last your lifetime,” said Cohen.
Once all the data is gathered, Stryker bundles it into a plan for the surgery that is sent to the surgeon.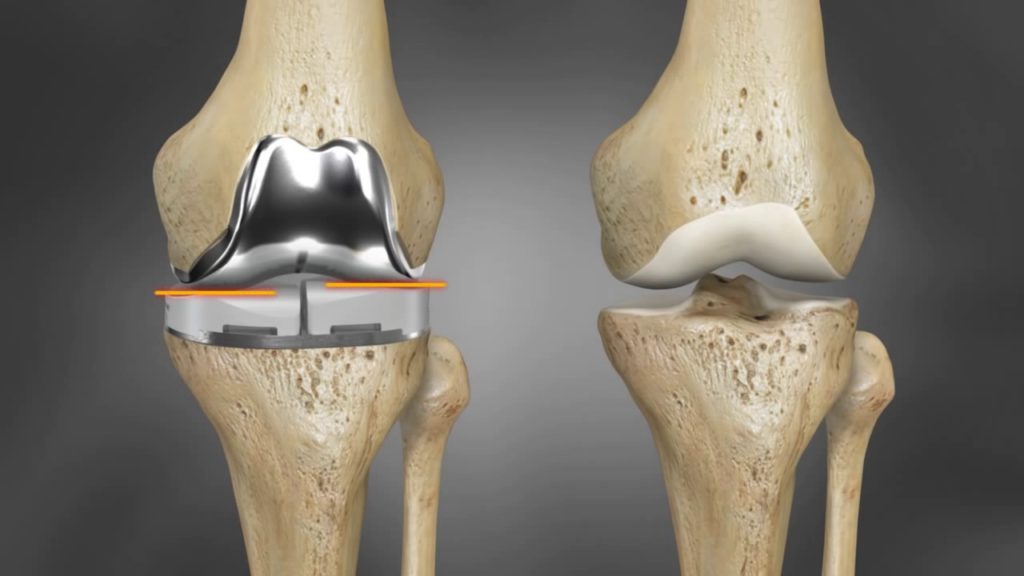 The plan is loaded into the robot before the patient enters the operating room. But it’s not the final surgical plan, Cohen pointed out. While the patient is under anesthesia, the surgeon bends the TKA knee and the robot tracks the bending action.
The plan is loaded into the robot before the patient enters the operating room. But it’s not the final surgical plan, Cohen pointed out. While the patient is under anesthesia, the surgeon bends the TKA knee and the robot tracks the bending action.
“So let’s say your ligaments are a little bit too loose, and the surgeon running the robot looks at the screen and says, ‘Ah, you know, the medial [collateral ligament] is a little bit lax. So we’re going to move the tibial component up a little bit, twist the femur, and now let’s flex the knee again—virtually—and see what the end surgery would look like in terms of flexion.’ ”
Once the plan has been fine-tuned and completely individualized, it’s locked in and surgery commences.
During the operation, the robot controls the motion of surgical instruments. For example, as the surgeon pushes a saw into a bone, the robot controls the plane of the blade and executes the cut with an accuracy and precision unseen in surgery before, said Cohen.
Robert Cohen, president of Stryker’s Digital, Robotics, and Enabling Technologies entity, has spent his entire career manufacturing prostheses.
The forward progress of the blade is controlled too. This prevents it from entering healthy tissue once the bone has been cut clean through. “We have haptics built into the robot arm,” said Cohen. “The saw stops automatically when you hit the bone’s boundary. We create a bubble, a safety zone.”
Better Outcomes
From the patient’s perspective, the biggest benefit of robot-assisted surgery is a shorter recovery time. This is largely a result of minimizing damage to healthy tissue and proper placement of the prosthetic.
Cohen said, “When you wake up [after surgery], you’re flexing in the right spot. You don’t have to relearn to walk, like in 1979 when implants were put in the wrong spot. Now you have less physical therapy sessions. You return to flexion earlier. You get relief from pain sooner because you didn’t have as much soft-tissue trauma. You can go back to work sooner. You don’t have any of the health issues.
You get relief from pain sooner because you didn’t have as much soft-tissue trauma. You can go back to work sooner. You don’t have any of the health issues.
“There are fewer re-admissions and re-operations. You have higher patient satisfaction.”
Personal Outcome
TKA surgery is major surgery. More “majorly” than I imagined before entering the hospital last November. (A bit of unsolicited advice: If you’re contemplating knee surgery, don’t watch a YouTube video of the procedure before the operation. Wait until after.) My biggest takeaway from the experience is that the return to mobility was much faster than expected.
My grandfather was bed-ridden for more than a week after his TKA surgeries. He spent weeks in rehabilitation before he was able to walk—with the aid of a walker. And although the implants greatly enriched his life, he needed two canes to get around for the rest of his days.
The circumstances surrounding my TKA surgery were different than my grandfather’s.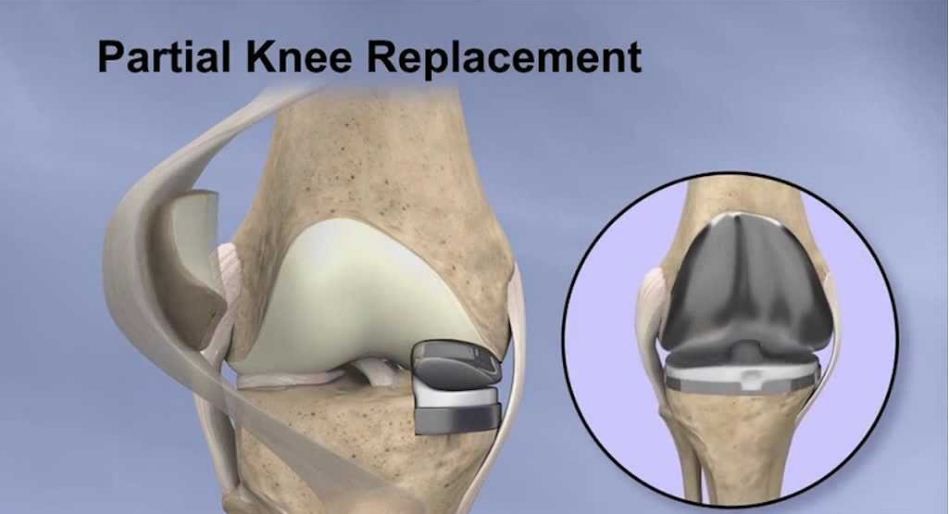 I was nearly 20 years younger, and I only had one knee operated on. I also was a “good” candidate for the surgery in that I was fit and had regularly done exercises to strengthen the muscles supporting the knee for the 15 years preceding the operation.
I was nearly 20 years younger, and I only had one knee operated on. I also was a “good” candidate for the surgery in that I was fit and had regularly done exercises to strengthen the muscles supporting the knee for the 15 years preceding the operation.
Still, eight hours after the procedure, I easily circumnavigated the orthopedic floor of the hospital with the assistance of a walker. I was discharged from the hospital 24 hours after surgery. And two days after the operation, on Thanksgiving Day, I was able to walk a half mile unaided.
It was a satisfying walk.
SIDEBAR
Knee implant surgery runs in the family
The Mako surgical robot helps prevent damage to healthy tissue and locates the knee implant correctly on the patient’s bones.
I’m not the first member of my family to take a prosthetic knee.
My grandfather had both knees replaced in 1979, at the age of 85. He became one of the earliest adopters of the then-rare procedure so he could continue to tend his garden. My mother-in-law had her knees replaced about 20 years ago, at 65, out of a desire to play tennis and tend to her grandchildren.
My mother-in-law had her knees replaced about 20 years ago, at 65, out of a desire to play tennis and tend to her grandchildren.
The reasons people choose to have total knee replacements today are different than they were 40 years ago. Robert Cohen, president of Stryker’s digital manufacturing entity, said the most common reason is to enhance mobility.
“Thirty years ago, a person 75 years old may have just wanted an implant to relieve pain,” he said. “Now, somebody 75, 80 years old wants to be able to walk a golf course ... sit on the floor with a grandkid and get up off the floor unaided.”
This desire has boosted the number of knee surgeries performed and attracted younger adults who want the procedure. Stryker has manufactured knees for individuals in their 40s, 30s, and even 20s, said Cohen. “We had someone who has a partial knee who rides in the Tour de France.”
No member of my family has qualified to compete for the yellow jersey, but those of us who have had the surgery were glad we did. My grandfather worked in his garden until he died, at 96, and my mother-in-law still plays tennis and keeps up as best she can with her now-adult grandchildren.
My grandfather worked in his garden until he died, at 96, and my mother-in-law still plays tennis and keeps up as best she can with her now-adult grandchildren.
My main reason for having the procedure was to continue my regimen of walking three to five miles a day without pain. Five months after surgery, I’m back to walking three miles daily pain-free. –D. Nelson
Hip arthroplasty using a 3D printer for the first time in Israel
In recent years, a real revolution has taken place in the field of joint replacement in the world. Increasingly, scientists are talking about the possibilities of 3D technologies, which make it possible to design an accurate three-dimensional model of a human organ in accordance with its anatomy in a computer and print it from biological material. For the first time in Israel, the Soroka hospital performed a knee replacement operation using a modeled and printed joint. nine0003
Author Elena Levina
When traditional treatments - physiotherapy, drug therapy - do not help, when joint pain turns into a constant, ongoing nightmare - perhaps the next step should be surgery to replace the affected joint.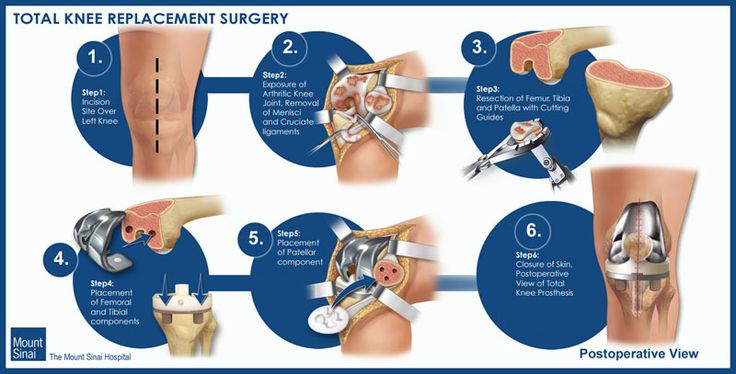 In recent years, a real revolution has taken place in the field of joint replacement in the world.
In recent years, a real revolution has taken place in the field of joint replacement in the world.
Medical revolution - 3D technology
Increasingly, scientists are talking about the possibilities of 3D technologies, which make it possible to design an accurate three-dimensional model of a human organ in accordance with its anatomy in a computer and print it from biological material. For the first time in Israel, the Soroka hospital performed a knee replacement surgery using simulation. nine0003
When a joint replacement is required
If joint pains are repeated, and you know that the reason for this is not physical exertion on the limbs, then most likely we are talking about one or another type of arthritis - inflammation. Most often, diseased joints are in the lower extremities, in the knees, and the hip bones. Sometimes the only solution is surgical replacement of damaged joints.
The average age of patients with recurrent joint pain, other than injury or accident, is approximately 60 years or older.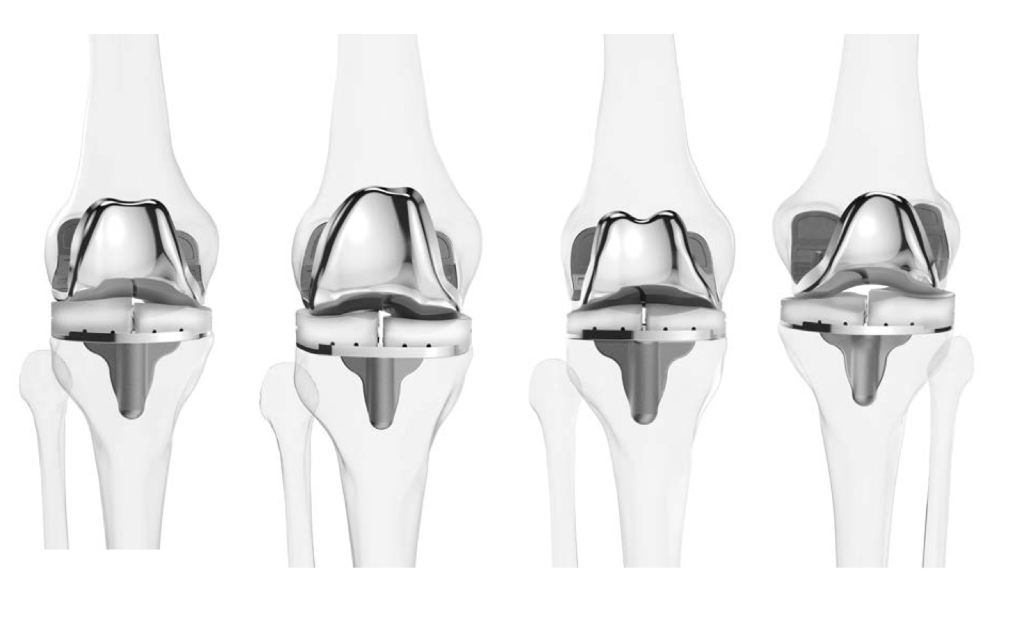 Due to natural wear and tear and degenerative processes in the body that occur with age. Joint replacements may also be needed for younger people who have suffered fractures and injuries from sports or accidents where surgery is the only option. nine0003
Due to natural wear and tear and degenerative processes in the body that occur with age. Joint replacements may also be needed for younger people who have suffered fractures and injuries from sports or accidents where surgery is the only option. nine0003
Joint replacement surgery with 3D printers already in Israel!
Ami Asis, a resident of the south of the country, was the first patient in Israel and one of the few in the world whose damaged joint was replaced with a new one created using a 3D printer. Ami, who for many years suffered from pain in the hip joint and lameness, had long dreamed of replacing the damaged joint, but he knew that such operations are very complex, require high qualification and experience from the doctor, complications are possible due to inaccurate selection of the implant . Dr. Vadim Benkovich, head of the arthroplasty department at the Soroka hospital in Beer Sheva, suggested that he implant a 3D-printed implant. After some hesitation, Ami agreed to the procedure. The operation was performed at Soroka Hospital in Beersheba and took about 30 minutes. nine0003
After some hesitation, Ami agreed to the procedure. The operation was performed at Soroka Hospital in Beersheba and took about 30 minutes. nine0003
One-on-one model
Creating a prosthesis in accordance with the individual measurements of the patient, which would exactly repeat the anatomy of his joint, is the basis of a new method of creating an implant using 3D printers. Before the operation, the patient undergoes visual scanning procedures: MRI and CT, but not for a diagnostic examination, for which these procedures are intended, but to recreate an accurate three-dimensional model of the joint. This creates a one-on-one model of the problematic organ to be replaced. This exact copy allows doctors to plan all actions to the smallest detail, to select the adapted equipment suitable for each specific case. Orthopedics in Israel is advancing by leaps and bounds - the doctors of the country have tried various methods of surgery and materials from which implants were created.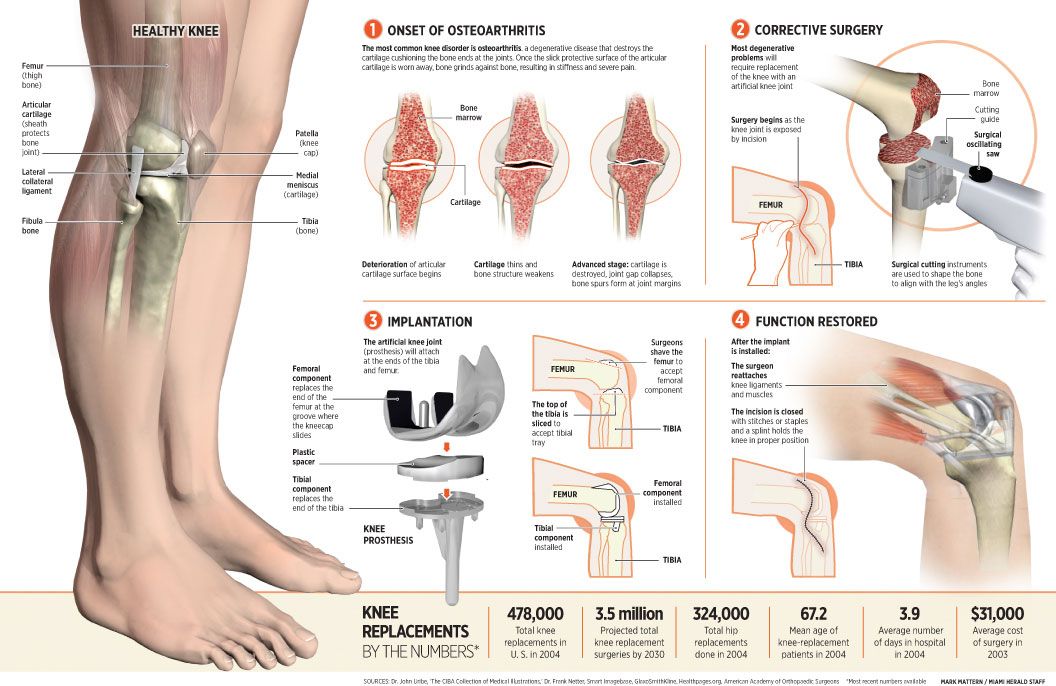 But the patient's recovery process was always very slow and painful. nine0003
But the patient's recovery process was always very slow and painful. nine0003
Benefits of using a 3D printer in orthopedics
The advantage of creating a joint model using a 3D printer is that it allows for a very high level of accuracy and reduces work time. This is important, first of all, because we are talking about the most precise "jewelry" operations, which are carried out in a short time and at a very high professional level. Speaking about the advantages of the method of joint replacement using "opened" organs, it is worth noting that, compared with previous methods, there are no traditional consequences of surgical intervention: tissue is less damaged, less blood loss, the patient recovers faster after surgery. In the case of Ami, we are talking about a fairly short time: only a month has passed since the surgery, he can already drive a car, move around, almost without limping, he has stopped taking analgesics for the last week. nine0003
Today, Israeli orthopedists are dreaming of the next stage - to perform the most complex spinal surgeries, requiring, for example, replacement of vertebrae, using 3D organ printing technologies.
Request a treatment quote
Watch video - 2:58 min.
D.R.A Medical Center
With D.R.A Medical Center you get the opportunity to use the services of the best Israeli doctors and receive effective treatment based on your individual needs at the most reasonable cost. Read more
Knee implants on a 3D printer: a new printing technique
Knee implants on a 3D printer
It is not news for a long time that one of the most useful areas of 3D printing for humans, in the future, is medicine. New ways of making prostheses and even organ fragments are constantly being developed. 3D printing can be extremely useful for surgeons and dentists. The development of this 3D printing industry does not stand still, researchers are hard at work on the invention of new printing methods in medicine and optimization of existing ones. For example, scientists create knee implants on a 3D printer that are significantly superior to their traditional counterparts. nine0003
nine0003
The American company ConforMIS, which specializes in the manufacture of knee prostheses, has developed a radical new technology iTotal. It allows you to create unique knee joints, which, thanks to 3D technologies, provide the ability to adapt to the characteristics of each individual. Knee implants on a 3D printer, created using this technology, contribute to faster healing of the operated area, reducing pain. They also provide greater mobility than standard prostheses currently used by surgeons. nine0003
3D printing of knee implants
The technology provided by ConforMIS is quite new, but has already proved to be very effective. Dr. Brian Guber, an American orthopedic surgeon formerly of ConforMIS's scientific advisory department, has been using the system for four years, long before it was widely publicized. During this time, he has gained an excellent reputation as a result of successful knee replacement surgeries; he accepted patients in need of surgery from all over the United States. nine0049 Recently, Dr. Guber invited reporters from the independent newspaper Seven Days to oversee one of the patella replacement procedures. The patient was a woman who had problems with her knees due to being overweight. Two months before the operation, a 3D scan of the patient's knee was performed to build a unique model in order to recreate an exact copy of the patella using a 3D printer. After removing the calyx, the doctor replaced it with a 3D printed cobalt-chromium alloy replica.
nine0049 Recently, Dr. Guber invited reporters from the independent newspaper Seven Days to oversee one of the patella replacement procedures. The patient was a woman who had problems with her knees due to being overweight. Two months before the operation, a 3D scan of the patient's knee was performed to build a unique model in order to recreate an exact copy of the patella using a 3D printer. After removing the calyx, the doctor replaced it with a 3D printed cobalt-chromium alloy replica.
3D printed knee implants were not the only thing custom made for the patient. Surgical instruments have also been designed specifically based on the female anatomy. Such a well-established and responsible approach to business allowed the doctor to complete the operation in less than an hour. Incredibly, the patient, having gone to the operation at about 10:30, was already able to walk by the evening.
Most of Dr. Huber's patients leave the hospital within 24-48 hours, which is clearly a much shorter time than is required with standard knee prostheses. He has operated on many overtrained athletes, and less than five percent of his patients require physical rehabilitation. nine0003
He has operated on many overtrained athletes, and less than five percent of his patients require physical rehabilitation. nine0003
The future of knee implants on a 3D printer
The benefits of the ConforMIS system are clear. Conventional knee implants are made to measure general anatomy. And this is unthinkable, given how different people can be from each other. According to Dr. Huber, two-thirds of replacement knee prostheses are either too big or too small, limiting mobility and causing chronic pain. In addition to making them generally unprofitable, conventional implants often require additional removal of significant bone fragments. 3D printed knee implants offer the opportunity to save 25-30 percent more bone than standard knee replacements, as well as significantly reduce blood loss. nine0003
The role of 3D printing in medicine is truly enormous and new opportunities for its application continue to appear every day. After all, no other technology would allow such an accurate reproduction of the unique parts of the patient's body, especially bones and internal organs.